Код МКБ-10
Z49.0 Подготовительные процедуры для проведения диализа
- при состояниях при острой почечной недостаточности (остром повреждении почек) N17 (N17.0; N17.1; N17.2; N17.8; N17.9)
- при состояниях при хронической болезни почек N18 (N18.4; 18.5)
Виды, формы, условия оказания медицинской помощи пациенту с данным заболеванием или состоянием
В рамках оказания специализированной медицинской помощи по профилю «нефрология» специальными методами лечения методами диализа, исходя из потребности и объема проводимой лечебной работы, подготовительные процедуры для создания доступа для диализа (сосудистого доступа для диализа и доступа для перитонеального диализа) пациентам при состояниях ХБП 5-й стадии и ОПП организуются врачами-нефрологами с привлечением врачей-рентгенологов, врачей ультразвуковой диагностики, врачей-хирургов; врачей-сердечно-сосудистых хирургов, врачей по рентгенэндоваскулярной диагностике и лечению, врачей-анестезиологов-реаниматологов, предусмотренных Номенклатурой специальностей.
Приказ № 700н Министерства здравоохранения Российской Федерации от 07.10.2015 (зарегистрирован Министерством юстиции Российской Федерации 12.11.2015, регистрационный номер № 39696) с изменениями, внесенными Приказом № 771н Министерства здравоохранения Российской Федерации от 11.11.2016 (зарегистрирован Министерством юстиции Российской Федерации 26.12.2016, регистрационный номер № 44926) (далее – Номенклатура специальностей).
Подготовительные процедуры для создания доступа для диализа (сосудистого доступа для диализа и доступа для перитонеального диализа) пациентам при состояниях при ОПП организуются в экстренной и неотложной формах в условиях, обеспечивающих круглосуточное медицинское наблюдение и лечение в рамках оказания специализированной медицинской помощи.
Подготовительные процедуры для создания доступа для диализа (сосудистого доступа для диализа и доступа для перитонеального диализа) пациентам при состояниях при ХБП 4-й или 5-й стадии организуются в экстренной и неотложной формах в условиях, предусматривающих медицинское наблюдение и лечение в дневное время, но не требующих круглосуточного наблюдения, или в условиях, обеспечивающих круглосуточное медицинское наблюдение и лечение в рамках оказания специализированной медицинской помощи.
Федеральный закон № 323-ФЗ «Об основах охраны здоровья граждан в Российской Федерации» от 21.11.2011
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016)
Аббревиатуры и сокращения
- Kt/V – доза диализа;
- MRSA — Метициллин-резистентный золотистый стафилококк;
- Staphylococcus aureus (S. аureus) – золотистый стафилококк;
- Pseudomonas aeruginosa – синегнойная палочка;
- АВ – артериовенозный;
- АВТ – артериовенозный трансплантат (синоним: АВ-трансплантат, синтетический сосудистый протез);
- АВФ – артериовенозная фистула (синоним: АВ-фистула, аутогенная или нативная фистула);
- ГД – гемодиализ;
- КАИК – катетер-ассоциированные инфекции кровотока;
- МКБ10 – международная классификация болезней 10-го пересмотра;
- нтЦВК – нетуннелированный, безманжеточный катетер;
- ОПП – острая почечная недостаточность (острое повреждение почек);
- ПД – перитонеальный диализ;
- тХПН – терминальная стадия хронической почечной недостаточности;
- тЦВК – туннелированный манжеточный катетер;
- УЗИ – ультразвуковое исследование;
- ХБП – хроническая болезнь почек;
- ХБП-5 – хроническая болезнь почек 5-й стадии;
- ЦВК – центральный венозный катетер;
- КТ – компьютерная томография.
Цель
Цель разработчиков клинических рекомендаций заключается в написании текущего клинического документа с практическими рекомендациями по доступу для диализа врачам-специалистам, которые входят в состав мультидисциплинарной команды по лечению пациентов методами диализа при состояниях при ОПП и ХБП 4–5-й стадий. Рекомендации заключаются в обобщении и оценке всех имеющихся в настоящее время доказательств по пред-, пери- и послеоперационной медицинской помощи по формированию, уходу и долгосрочному использованию доступа для диализа, чтобы помочь врачам-специалистам в выборе лучшей тактики лечения. Тем не менее каждый врач на основании своих знаний и компетенции должен принять окончательное решение относительно индивидуального подхода к пациенту. Этот документ не набор правил, а руководство к действию в определенных ситуациях, позволяющее гибко подходить к ситуациям при конкретных условиях и состоянии пациента.
В рекомендациях изложены принципы профилактики и ухода за доступом для диализа, правила формирования доступа для диализа. Предназначены всем медицинским работникам вне зависимости от профиля и места оказания медицинской помощи, а также студентам, аспирантам и преподавателям медицинских вузов и системы последипломного медицинского образования.
Целевая аудитория клинических рекомендаций:
- врачи-анестезиологи-реаниматологи;
- врачи-педиатры;
- врачи-неонатологи;
- врачи-рентгенологи;
- врачи ультразвуковой диагностики;
- врачи-сердечно-сосудистые хирурги;
- врачи по рентгенэндоваскулярной диагностике и лечению;
- врачи скорой медицинской помощи;
- врачи-терапевты;
- врачи-инфекционисты;
- врачи-нефрологи;
- врачи-хирурги;
- врачи-эпидемиологи;
- медицинские сестры;
- медицинские сестры перевязочные;
- медицинские сестры процедурные;
- операционные медицинские сестры;
- помощники врача-эпидемиолога;
- преподаватели учебных заведений;
- аспиранты;
- ординаторы;
- студенты.
Термины и определения
Доступ для диализа – это общий термин, включающий функционирующий сосудистый или перитонеальный доступ, сформированный при помощи хирургического вмешательства или чрескожного введения катетера и обеспечивающий оказание медицинской помощи методом диализа при состояниях при ХБП 5-й стадии, при состояниях при ОПП.
Сосудистый доступ для диализа – это общий термин, включающий АВ-доступ и ЦВК для гемодиализа.
АВ-доступ – это общий термин, включающий АВ-фистулы и АВ-трансплантаты.
Первичный АВ-доступ – это создание функционирующего АВ-доступа впервые.
Вторичный АВ-доступ – это создание нативной АВ-фистулы или АВ-трансплантата в любом местоположении после неудачного первичного сосудистого доступа (исключая третичный сосудистый доступ).
Третичный АВ-доступ – это создание АВ-доступа с использованием большой подкожной или бедренной вен, транслоцированных на руку или ногу. Атипичные АВ-доступы включены в эту категорию.
АВ-фистула – это аутогенный сосудистый доступ, сформированный при помощи хирургического вмешательства для оказания медицинской помощи методом гемодиализа при состояниях при ХБП-5, представляющий собой анастомоз между артерией и веной, где часть вены выступает в качестве доступа для канюлирования (синоним: нативная АВ-фистула).
АВ-трансплантат – это сосудистый доступ, сформированный при помощи хирургического вмешательства для оказания медицинской помощи методом гемодиализа при состояниях при ХБП-5, созданный с помощью искусственного или биологического трансплантата, соединяющего артерию и вену, при этом сегмент трансплантата выступает в качестве доступа для канюлирования.
Созревание – это процесс преобразования анатомических структур и физиологических процессов организма, делающий вновь создаваемый АВ-доступ пригодным для канюлирования. Он включает увеличение диаметра АВФ, изменение структуры стенки вены, увеличение кровотока, инкорпорацию тканей в структуру АВ-трансплантата, отсутствие тромбоза и кровотечения как механизмов несостоятельности АВ-доступа (синоним: пригодность для оказания медицинской помощи методами гемодиализа, диализа).
Зрелый АВ-доступ – это сосудистый доступ, обеспечивающий достаточный кровоток, подходит для канюляции двумя иглами при оказании медицинской помощи специальными методами лечения (гемодиализ).
Функционирующий АВ-доступ – это сосудистый доступ, который обеспечивает достижение адекватной дозы гемодиализа и предписанный эффективный средний кровоток >300 мл/мин при канюляции двумя иглами, при оказании медицинской помощи специальными методами лечения (гемодиализ) в течение не менее 6 последовательных процедур.
Транспозиция – это перемещение аутогенной вены в новое (более поверхностное) положение в мягких тканях той же анатомической области.
Транслокация – это манипуляция для создания АВ-фистулы, при которой подготовленная вена полностью отключена и перемещается в новую анатомическую область.
Суперфициализация – это когда вена доступа транспонируется в подкожно-жировую клетчатку и расположена ближе к коже.
Канюлирование – это введение игл для диализа в АВ-доступ с лечебной целью, обеспечивающее подключение больного к аппарату искусственная почка.
Клинический мониторинг – это регулярная клиническая оценка АВ-доступа через определенные интервалы времени; отличается от инструментальных методов исследования, включает оценку вибрации (колебания, дрожания) и шума в области АВ-доступа, оценку продолжительности гемостаза после удаления иглы и оттока после подъема руки.
Наблюдение АВ-доступа – это универсальный термин, включающий как клиническую оценку, так и инструментальные методы исследования АВ-доступа, в том числе параметры процедуры гемодиализа, такие как средняя эффективная скорость кровотока, динамическое изменение трансмембранного давления и давления в сегменте артерии и вены на блоке аппарата «искусственная почка», доза диализа (Kt/V); последовательные измерения динамики потока в области доступа с анализом тренда; рециркуляция в АВ-доступе или дуплексное сканирование АВ-доступа.
Техническое наблюдение – это регулярная экспертиза и оценка АВ-доступа при помощи инструментальных методов исследования через определенные интервалы времени; следует отличать от клинического мониторинга.
Рециркуляция – это многократное полное или частичное возвращение потока крови в технологический процесс с целью регулирования гомеостаза.
Тромбоз АВ-доступа – это формирование внутри АВ-доступа тромбов с утратой анатомической, гемодинамической и клинической проходимости АВ-доступа, препятствующих свободному току крови.
Отказ АВ-доступа – это когда АВ-доступ стал окончательно непригодным по тем или иным причинам или не пригодным для канюлирования.
Индуцированная АВ-доступом ишемия конечностей – это неправильная перфузия конечностей после создания АВ-доступа.
Превентивное вмешательство – это вмешательство, направленное на устранение стеноза или иной проблемы АВ-доступа, продолжающего обеспечивать адекватную дозу диализа; цель вмешательства – предотвратить нарушение функции АВ-доступа.
Первичная несостоятельность АВ-доступа – это АВ-доступ, который, несмотря на рентгенэндоваскулярное или хирургическое вмешательство, не может быть успешно использован для оказания медицинской помощи методами гемодиализа к установленному моменту времени (обычно сверх 3 месяцев) после формирования (синоним: невозможность использования для диализа).
Первичная самостоятельная проходимость – это интервал между формированием АВ-доступа или его расположением до первого вмешательства (рентгенэндоваскулярного или хирургического) для поддержания или восстановления кровотока или до первого эпизода тромбоза АВ-доступа (синоним: сохранность АВ-доступа без вмешательства; первичная проходимость).
Первичная функциональная проходимость – это интервал между первым использованием вновь созданного АВ-доступа и первым повторным вмешательством для спасения сосудистого доступа или отказа от его использования.
Вторичная проходимость – это время от формирования АВ-доступа или его расположения до отказа от АВ-доступа либо необратимая утрата АВ-доступа (синоним: совокупная выживаемость АВ-доступа).
Катетеризация центральных вен – это чрескожное введение катетера в одну из центральных вен с лечебной целью. Термин, используемый в англоязычной литературе, близкий по смыслу: Catheter Placement.
Центральный венозный катетер для диализа (гемодиализа) – это катетер, используемый в медицине для катетеризации центральных вен, имеющий на конце одно или несколько отверстий и обеспечивающий подключение больного к аппарату «искусственная почка». В качестве сосудистого доступа для экстракорпорального используются нетуннелированный и туннелированный (манжеточный). Термин, используемый в англоязычной литературе, близкий по смыслу: central vascular catheter for dialysis, CVC access for dialysis.
Нетуннелированный центральный венозный катетер – это катетер, кратковременно используемый в качестве сосудистого доступа для экстракорпорального диализа. Дизайн постепенно эволюционировал, катетеры имеют, как правило, два разделенных просвета для артериального и венозного кровотоков, как правило, без манжеты, конические, жесткие; вводятся через проводник. Термин, используюемый в англоязычной литературе, близкий по смыслу: non-tunneled temporary hemodialysis catheters (NTHCs).
Туннелированный центральный венозный катетер – это катетер, используемый в качестве сосудистого доступа для экстракорпорального диализа, для длительной терапии по замещению функции почек специальными методами лечения. Как правило, с подкожным устройством для фиксации катетера (манжета) и имеет один просвет для оттока крови («артериальный») и один – для возврата крови («венозный»). Термин, используемый в англоязычной литературе, близкий по смыслу: Tunneled Hemodialysis Catheters.
Первичная проходимость катетера – это интервал между введением катетера и первым вмешательством для восстановления функции катетера.
Вторичная проходимость катетера – это интервал между введением катетера и обменом или удалением катетера по какой-либо причине.
Постоянный доступ катетер – это интервал между введением катетера и отказом от использования катетера в качестве доступа по любой причине, включая периоды времени после обменов катетера в том же сосуде. Период времени и количество обменов документированы, например 12 месяцев [3 катетера].
Дисфункция катетера для диализа – это нарушение функционирования доступа для диализа, которое определяется как невозможность завершения процедуры диализа через ЦВК для диализа из-за повторяющихся сигналов тревоги; достижения эффективного среднего кровотока >300 мл/мин (при этом Ра и Рв на блоке аппарата «искусственная почка» в целевых значениях), в двух последовательных процедурах диализа; достижения Kt/V ≥1,2 за 4 часа. Дисфункция катетера констатируется только в том случае, если она сохраняется, несмотря на попытки изменить положение пациента; изменить подключение к портам катетера артериальной и венозной магистрали; принудительного промывания катетера. Должны быть исключены все проблемы, связанные с медицинским персоналом и преципитацией медикаментов.
Колонизация катетера – значимый рост культуры микроорганизмов с порта, подкожного сегмента или с дистального конца катетера.
Инфекция места выхода катетера – это наличие выделений или эритемы, уплотнения и/или болезненности в месте выхода катетера положительной бактериологической диагностикой культуры из серозных выделений (возможно, клинические признаки инфекции с отрицательными результатами культуры из выделений и крови) без признаков раздражения от повязки, шовного материала или средств для обработки кожных покровов.
Туннельная инфекция, связанная с катетером, – это наличие гнойных выделений из туннеля или эритемы, уплотнения и/или болезненности в проекции на кожу туннеля с положительной бактериологической диагностикой культуры (возможно, клинические признаки инфекции с отрицательными результатами культуры из выделений и крови).
Катетер-ассоциированная инфекция кровотока, связанная с доступом для диализа (КАИК),– это группа инфекционных заболеваний, развивающихся у пациента при состояниях при ХБП-5, при состояниях ОПП, в результате использования катетера в качестве сосудистого доступа при оказании медицинской помощи методами экстракорпорального диализа. КАИК – это клиническое определение, которое используется для диагностики и лечения пациентов и требует специального лабораторного подтверждения для более тщательного выявления катетера для экстракорпорального диализа как источника инфекции кровотока. Определяется как рост одного и того же организма из катетера для экстракорпорального диализа и периферической вены (или из экстракорпоральной системы для диализа) пациента с клиническими признаками инфекции и без альтернативного источника инфекции кровотока. Термин, используемый в англоязычной литературе, близкий по смыслу: Catheter-related bloodstream infection (CRBSI). catheter related bacteremia (CRB), access related bloodstream infection.
Катетер для перитонеального диализа – это специальный катетер, используемый в медицине в качестве доступа для перитонеального диализа, имеющий на конце несколько отверстий, обеспечивающий адекватную скорость потока втекающего и вытекающего растворов, как правило, имеющий устройства для фиксации катетера, минимизирующие инфицирование. Термин, используемый в англоязычной литературе, близкий по смыслу: Peritoneal dialysis catheter.
Имплантация катетера для перитонеального диализа – это введение катетера в брюшную полость с лечебной целью. Термин, используемый в англоязычной литературе, близкий по смыслу: peritoneal catheter implantation.
Осложнения, связанные с катетером для перитонеального диализа, – это группа механических и инфекционных осложнений, развивающихся у пациента при состояниях при ХБП-5, при состояниях при ОПП, в результате использования катетера в качестве доступа при оказании медицинской помощи методами перитонеального диализа. Термин, используемый в англоязычной литературе, близкий по смыслу: peritoneal catheter complications.
Перикатетерное протекание – это протечки диализата через брюшную стенку вдоль катетера для перитонеального диализа в подкожные ткани, может диагностироваться как неожиданное снижение обычного объема слива и вызывать предположение о снижении ультрафильтрации, имитировать гипергидратацию. Термин, используемый в англоязычной литературе, близкий по смыслу: pericatheter leak.
Нарушение функции перитонеального катетера – это несостоятельность дренажа, обычно выявляемая, когда объем сливаемого диализата существенно ниже, чем объем заливки, и нет данных о наличии перикатетерного протекания. Термин, используемый в англоязычной литературе, близкий по смыслу: peritoneal catheter malfunction.
Инфекция, связанная с катетером для перитонеального диализа,– это группа инфекционных заболеваний, развивающихся у пациента при состояниях при ХБП-5, при ОПП, в результате использования катетера в качестве доступа при оказании медицинской помощи методами перитонеального диализа. Термин, используемый в англоязычной литературе, близкий по смыслу: catheter infection.
Инфекция места выхода катетера для перитонеального диализа – это болезненность, гиперемия и/или отек/уплотнение тканей вокруг места выхода катетера без сопутствующей туннельной инфекции и перитонита. Термин, используемый в англоязычной литературе, близкий по смыслу: tunnel infection
Туннельная инфекция катетера для перитонеального диализа – это болезненность, гиперемия и/или отек/уплотнение тканей вокруг подкожного сегмента катетера без сопутствующего перитонита. Термин, используемый в англоязычной литературе, близкий по смыслу: tunnel infection
Диализ – это замещение утраченной функции почек экстра- или интракорпоральными специальными методами лечения через сформированный доступ. Термин, используемый в англоязычной литературе, близкий по смыслу: Care involving dialysis.
Экстракорпоральный диализ – это специализированный полуселективный мембранный метод диализа с использованием аппаратов «искусственная почка», основанный на принципе переноса через полупроницаемую мембрану, изготовленную из естественных или синтетических материалов, воды и растворенных в ней молекул за счет градиентов концентрации и давления. Забираемая из сосудистого доступа кровь циркулирует через экстракорпоральный контур, состоящий из магистралей и фильтра. Во время процедуры в фильтре происходит эффективное удаление из крови воды и низкомолекулярных компонентов крови, токсических веществ и продуктов метаболизма, нормализация нарушений водного и электролитного баланса. Белки, форменные элементы крови, бактерии и вещества с молекулярной массой более 30 тыс. через мембрану не проходят. Очищенная кровь затем возвращается в организм больного через сформированный сосудистый доступ. Термин, используемый в англоязычной литературе, близкий по смыслу: Extracorporeal dialysis.
Перитонеальный диализ – это специальный интракорпоральный метод очищения крови, основан на принципе уравновешивания концентраций веществ в растворе, вводимых в брюшную полость, и кровью, припекающей и оттекающей от брюшины, с постепенным и непрерывным очищением крови от эндогенных и экзогенных токсинов, с одновременной коррекцией водно-солевого баланса, метаболических расстройств путем диффузии и фильтрации веществ через брюшину. Процесс заливки диализата и его удаление выполняются периодически ручным способом. Использование интермиттирующего перитонеального диализа предусматривает имплантацию специального катетера в брюшную полость. Термины, используемые в англоязычной литературе, близкие по смыслу: Peritoneal dialysis (PD) – перитонеальный диализ; Intermittent PD –интермиттирующий (прерывистый) ПД; Continuous Equilibration PD – непрерывный (постоянный) равновесный ПД; Other dialysis – Peritoneal dialysis.
Перитонеальный диализ с использованием автоматизированных технологий – это специальный интракорпоральный метод очищения крови, основан на принципе постепенного и непрерывного очищения крови от эндогенных и экзогенных токсинов с одновременной коррекцией водно-солевого баланса, метаболических расстройств путем диффузии и фильтрации веществ через брюшину как естественную полупроницаемую мембрану. Использование перитонеального диализа с использованием автоматизированных технологий предусматривает имплантацию специального катетера в брюшную полость. Процесс заливки диализата и его удаление автоматизированы при помощи аппарата – циклера. Термин, используемый в англоязычной литературе, близкий по смыслу: Automated PD – автоматизированный ПД; Adapted PD (APD) – адаптированный ПД; Continuous Equilibration PD – непрерывный (постоянный) равновесный ПД; высокообъемный ПД – High volume peritoneal dialysis HVPD; Continuous cycler assisted PD (CCPD) — постоянный циклерный ПД; Tidal PD – приливной ПД.
АКТУАЛЬНОСТЬ ПРОБЛЕМЫ
Эффективное лечение пациентов на современном этапе при состояниях терминальной стадии хронической почечной недостаточности (хронической болезни почек 5-й стадии – далее ХБП-5), при состояниях острой почечной недостаточности (остром повреждении почек, далее – ОПП) неразрывно связано с необходимостью создания доступа для организации терапии по замещению функции почек специальными методами лечения. Надежно функционирующий доступ остается ключевым, фундаментальным компонентом адекватного диализа. Идеальный доступ должен обеспечить безопасную и эффективную терапию, достаточную дозу диализа, быть простым и надежным в использовании, неся минимальный риск для пациента, получающего специализированную медицинскую помощь по профилю нефрологии специальными методами лечения (диализ). Индивидуальный подход к созданию доступа к диализу с учетом интересов пациента играет важную роль в улучшении удовлетворенности пациентов и клинических результатов. Выбор оптимального доступа к отдельному пациенту и определение сроков создания доступа зависят от наличия множества факторов, которые могут варьироваться в широких пределах для каждого пациента, включая демографию, сопутствующие заболевания, анатомию и личные предпочтения. Часто решение о типе доступа зависит от состояния пациента, желаемого качества жизни и жизненных целей. Раннее планирование и сохранение сосудов помогут сформировать идеальный сосудистый доступ для данного пациента.
National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for 2006 Updates: Hemodialysis Adequacy, Peritoneal Dialysis Adequacy and Vascular Access. American journal of kidney diseases. 2006;48:S1—S322.
Tordoir J., Canaud B., Haage P. et al. EBPG on Vascular Access. Nephrology Dialysis Transplantation. 2007;22:ii88—117.
Francis D., Van Schie D., Irish A. et al. Part 1 Dialysis Guidelines – Vascular Access. The CARI Guidelines – Caring for Australians with Renal Impairment, J. Knight et al., Editors. 2000, Excerpta Medica Communications. 2000: Sydney. Р. 10, 16.
Grace B., Hurst K., and McDonald S., Chapter 1. Stock and Flow., in Australia and New Zealand Dialysis and Transplant Registry, thirty fourth annual report., S. McDonald and K. Hurst, Editors. 2011: Adelaide, South Australia.
Fistula First Catheter Last Initiative: Available at: http://esrdncc. org/ffcl/. Accessed December 9, 2016.
Drew D.A., Lok C.E. Strategies for planning the optimal dialysis access for an individual patient. Curr Opin Nephrol Hypertens. 2014 May;23(3):314–320. Doi: 10.1097/01.
Золотым стандартом является высококачественная нативная артериовенозная фистула (АВ-фистула), доступная для большинства пациентов. АВ-фистула долговечна, отличается самым низким уровнем осложнений, не требует значимых дополнительных вмешательств, экономична. Многие, если не все, профессиональные сообщества нефрологов в настоящее время рекомендуют АВ-фистулу как предпочтительный сосудистый доступ к гемодиализу. При использовании АВ-фистулы отмечен более низкий риск фатального исхода по сравнению с другими видами доступа для диализа.
Ravani P., Palmer S.C., Oliver M.J., Quinn R.R., MacRae J.M., Tai D.J., et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol 2013;24:465–473.
В погоне за максимизацией распространения АВФ мало внимания уделяется индивидуальному подходу. У пациентов пожилого возраста и/или пациентов с тяжелыми сопутствующими заболеваниями и ограниченностью продолжительности жизни и/или из-за анатомии сосудов создание АВФ – вопрос спорный. Индивидуальный подход к созданию доступа с учетом интересов пациента играет важную роль в улучшении удовлетворенности пациентов и клинических результатов.
Drew D.A., Lok C.E. Weiner D.E. Vascular Access Choice in Incident Hemodialysis Patients: A Decision Analysis J Am Soc Nephrol. 2015 Jan;26(1):183–191. Doi: 10.1681/ASN.2013111236. Epub 2014 Jul 25.
Amanda Gomes A., Schmidt R., Wish J. Re-envisioning Fistula First in a patient-centered culture. Clin J Am Soc Nephrol. 2013 Oct;8(10):1791–1797. Doi: 10.2215/CJN.03140313. Epub 2013 Jun 6.
Артериовенозные имплантаты, выполненные из синтетического или биологического материала, применяются при невозможности формирования АВ-фистулы.
Хотя использование центральных венозных катетеров (ЦВК) в качестве сосудистого доступа клиническими рекомендациями различных профессиональных сообществ во многих странах в настоящее время не приветствуется, доля пациентов, использующих их как жизненно важную опцию, продолжает оставаться повсеместно высокой, с преобладающим использованием пациентами, начинающими получать медицинскую помощь методами диализа. Простота введения и возможность их использования сразу, функционирование в течение нескольких месяцев в качестве сосудистого доступа для диализа, предпочтение пациента, выбор локализации, отсутствие кардиопульмональной рециркуляции, избежание чрескожной канюляции при каждом лечении дают ЦВК определенное преимущество над АВ-фистулой и АВ-трансплантатом.
Центральные венозные катетеры (как туннелированные, так и нетуннелированные, безманжеточные) устанавливаются пациентам без постоянного доступа при потребности в экстренном гемодиализе, при недостаточно отрегулированном планировании начала диализа (позднем направлении на лечение), в отсутствие додиализного наблюдения нефрологом, на время формирования или коррекции АВ-доступа. Однако этот доступ может быть единственно доступным пациентам, у которых создание или реконструкция фистулы или сосудистого имплантата представляется технически сложным, рискованным или невозможным, лицам более старшего возраста с сердечно-сосудистыми заболеваниями и/или с сахарным диабетом. Отчасти это может способствовать использованию ЦВК в качестве основного доступа для диализа.
Douglas M. Silverstein, Scott O. Trerotola, Timothy Clark, Garth James, Wing Ng, Amy Dwyer, Marius C. Florescu, Roman Shingarev, Stephen R. Ash and on behalf of the Kidney Health Initiative HDF Workgroup Clinical and Regulatory Considerations for Central Venous Catheters for Hemodialysis CJASN December 2018, 13(12) 1924–1932; Doi: https://doi.org/10.2215/CJN.14251217.
Mokrzycki M.H., Lok C.E. Traditional and non-traditional strategies to optimize catheter function: go with more flow. Kidney Int. 2010 Dec;78(12):1218–1231. Doi: 10.1038/ki.2010.332. Epub 2010 Sep 29.
Dhruve M.J., Chan C.T. Vascular Access in the Elderly: Does One Size Fit All? Am J Nephrol. 2017;45(6):484–485. Doi: 10.1159/000476005. Epub 2017 May 17.
При выборе медицинской помощи методами диализа профессиональное сообщество нефрологов в настоящее время рекомендует применять интегрированный подход, учитывающий преимущества перитонеального диализа в отсутствие медицинских противопоказаний. Центральное место в успешной терапии методами перитонеального диализа (ПД) занимает безопасное своевременное установление и поддержание функционирования надежного доступа для перитонеального диализа.
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor. Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
ЭПИДЕМИОЛОГИЯ ДОСТУПА ДЛЯ ДИАЛИЗА
Болезни почек – это глобальная проблема здравоохранения, от которой страдают более 750 млн (9,8%) человек во всем мире. Важность болезней почек (включая ОПП и ХБП) еще не получила в мире широкого признания, что делает эти заболевания забытым в повестке дня глобальной политики. Возможно, в скором времени болезни почек смогут привести к большему числу фатальных исходов, чем четыре основных: сердечно-сосудистые, онкологические, хронические респираторные заболевания и сахарный диабет. В 2015 г. около 1,2 млн человек с ХБП умерли. Более 2 млн человек в мире умерли в 2010 г. из-за отсутствия доступа к диализу.
GBD, 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1459–544.
Более 1,7 млн человек умирают от ОПП ежегодно.
Liyanage T., Ninomiya T., Jha V. et al. Worldwide access to treatment for end-stage kidney disease: A systematic review. Lancet 2015;385:1975–1982.
Mehta R.L., Cerda J., Burdmann E.A. et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): A human rights case for nephrology. Lancet 2015; 385: 2616–2643.
В течение последнего десятилетия во всем мире наблюдается устойчивый рост пациентов (более 2 млн), получающих лечение методами диализа, которым требуется создание и/или поддержание адекватного функционирования доступа к диализу. Остаются большие региональные различия в количестве созданных доступов для диализа и вероятности успешного их использования между Европой, Канадой и США даже после корректировки на особенности и клиническое состояние пациента. Уход за доступом характеризуется схожими проблемами с неменьшей значимостью.
Gallieni M., Saxena R., Davidson I. Dialysis access in Europe and North America: are we on the same path? Semin Intervent Radiol 2009;26:96–105.
Ethier J., Mendelssohn D.C., Elder S.J., Hasegawa T., Akizawa T., Akiba T., et al. Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant 2008;23:3219–3226.
Fissell R.B., Fuller D.S., Morgenstern H., Gillespie B.W., Mendelssohn D.C., Rayner H.C., et al. Hemodialysis patient preference for type of vascular access: variation and predictors across countries in the DOPPS. J Vasc Access 2013;14: 264–2672.
Международные тенденции определяют сосудистый доступ (70–90%) как основной к диализу во всем мире.
Anil K., Agarwal, Nabil J. Haddad, Tushar J. Vachharajan. Arif Asif Innovations in vascular access for hemodialysis. Kidney International (2019) 95, 1053–1063; https://doi.org/10.1016/ j.kint.2018.11.046
Усилия мирового нефрологического сообщества направлены на создание АВ-фистулы как первого доступа к диализу.
Arteriovenous fistula first website [20.09.2016]. Available from: www.fistulafirst.org
Раннее направление пациентов ХБП к нефрологу может свести к минимуму использование катетеров, уменьшить осложнения, связанные с ним, и необходимость госпитализации.
Davidson I., Gallieni M., Saxena R., Dolmatch B. A patient centered decision-making dialysis access algorithm. J Vasc Access 2007;8:59–68.
Когда гемодиализ служит методом выбора пациента, время от направления нефролога к хирургу для создания сосудистого доступа должно быть как можно короче. Время ожидания операции наряду со временем от создания АВ-доступа до первой канюляции значительно влияло на возможность оказания медицинской помощи методами диализа с постоянным сосудистым доступом. Среднее время от направления до создания АВ-доступа варьировалось от 5–6 дней в Италии, Японии ёи Германии до 40–43 дней в Великобритании и Канаде.
Ethier J., Mendelssohn D.C., Elder S.J., Hasegawa T., Akizawa T., Akiba T., et al. Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant 2008;23:3219–3226.
В подавляющем большинстве отделений/центров гемодиализа в России в 2015 г. в качестве сосудистого доступа использовалась нативная АВФ (88,0% от числа всех больных), 3,6% – АВ-трансплантат, 5,4% – туннелированный центральный венозный катетер, временный сосудистый доступ использовался в 3,0%, в целом соотношение этих видов сосудистого доступа практически не отличалось от такового в 2012–2013 гг. Среди больных с постоянным сосудистым доступом первичный доступ (АВ-фистула) на 31.12.2015 имели 63,6% больных, что мало отличалось от показателей предыдущих лет. Повторно созданный или реконструированный доступ был у 36,4% больных. В 2015 г. была выполнена 9261 операция (из них 56,8% по созданию первичного доступа и 43,2% повторных или реконструктивных операций). На каждого больного (пролеченного в отделениях, от которых была получена обсуждаемая информация) приходилось в среднем 0,38 операции в год (из них 0,21 первичной операции и 0,16 повторной и реконструктивной операции), что полностью соответствует показателям 2009–2013 гг.
Томилина Н.А., Андрусев А.М., Перегудова Н.Г. и соавт. Заместительная терапия терминальной хронической почечной недостаточности в Российской Федерации в 2010–2015 гг. Отчет по данным Общероссийского регистра заместительной почечной терапии Российского диализного общества, Часть первая «Нефрология и диализ». 2017. 19(4 – Приложение): 1–95. Doi: 10.28996/1680-4422-2017-4suppl-1-95.
Несмотря на это, пациенты реже стали использовать АВ-фистулу по сравнению с другими типами сосудистого доступа, особенно если пациент женского пола, более старшего возраста, имеющий больший индекс массы тела, имеющий в анамнезе сахарный диабет и периферическое сосудистое заболевание.
Почти 80% инцидентных пациентов в мире, начинающих экстракорпоральный диализ при состояниях ХБП-5, используют туннелированный катетер в качестве своего первого сосудистого доступа. Уровень использования катетера остается неизменным на протяжении многих лет. Частота использования ЦВК превалентными пациентами колеблется около 20%. Это, безусловно, превышает опубликованные рекомендации (например, NKF-KDOQI – менее 10%). Saran R., Robinson B., Abbott K.C., et al. US renal data system 2017 annual data report: Epidemiology of kidney disease in the United States. Am J Kidney Dis. 2018;71(3):A7.
Rayner H.C., Pisoni R.L. The increasing use of hemodialysis catheters: evidence from the DOPPS on its significance and ways to reverse it. Semin Dial. 2010;23:6.
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis. 2004;44:779.
Polkinghorne K., Dent H., Gulyani A. et al, Chapter 5: Haemodialysis, in Australia and New Zealand Dialysis and Transplant Registry. Thirty fourth annual report., S. McDonald and K. Hurst, Editors. 2011: Adelaide, South Australia.
CORR 2010 CORR Report–Treatment of End-Stage Organ Failure in Canada, 1999 to 2008, 2010.
USRDS: 2015 USRDS annual data report, volume 2: End-stage renal disease. Available at: https://www.usrds.org/2015/download/vol2_USRDS_ESRD_15. Accessed August 1, 2016.
National Kidney Foundation K/DOQI clinical practice guidelines for vascular access: Update 2000. Am J Kidney Dis. 2001;37:S137-S181. Available at: http://www.kidney.org/professionals/KDOQI/ guideline_up HD_PD_VA /index. htm. Accessed April 2, 2012.
Mickley V. Steal syndrome-strategies to preserve vascular access and extremity. Nephrology Dialysis Transplantation. 2008; 23: 19–24.
Ravani P., Palmer S.C., Oliver M.J. et al. Associations between Hemodialysis Access Type and Clinical Outcomes: A Systematic Review. Journal of the American Society of Nephrology. 2013; 24: 465–473.
Xue H., Ix J.H., Wang W., Brunelli S.M., Lazarus M., Hakim R., Lacson E. Jr. Hemodialysis access usage patterns in the incident dialysis year and associated catheter-related complications. Am J Kidney Dis. 2013 Jan;61(1):123–130. Doi: 10.1053/j.ajkd.2012.09.006. Epub 2012 Nov 16.
Предпочтение пациентов ЦВК в качестве доступа к диализу варьировалось по странам: от 1% в Японии и 18% в США до 42–44% в Бельгии и Канаде, и связано с возрастом, женским полом, бывшим или текущим использованием катетера; предпочтение пациента может зависеть от социально-культурных факторов.
Fissell R.B., Fuller D.S., Morgenstern H., Gillespie B.W., Mendelssohn D.C., Rayner H.C., et al. Hemodialysis patient preference for type of vascular access: variation and predictors across countries in the DOPPS. J Vasc Access 2013;14:264–272.
В пяти странах отмечается преобладание ЦВК в качестве доступа для начала диализа, несмотря на то что пациенты были под наблюдением нефролога более 4 месяцев. Использование катетера как сосудистого доступа для диализа выросло в 1,5–3 раза среди пациентов без сахарного диабета в возрасте от 18 до 70 лет при состояниях при ХБП-5, получающих медицинскую помощь методами диализа во многих странах с 1996 по 2007 г.
Ethier .J, Mendelssohn D.C., Elder S.J., Hasegawa T., Akizawa T., Akiba T., et al. Vascular access use and outcomes: an international perspective from the Dialysis Outcomes and Practice Patterns Study. Nephrol Dial Transplant 2008;23:3219–3226.
Мировое сообщество по нефрологии предлагает использовать стандартный центральный венозный двухпросветный нетуннелированный катетер для гемодиализа в качестве сосудистого доступа для начала лечения методами экстракорпорального диализа взрослым пациентам при критических состояниях и при остром повреждении почек. Однако в настоящее время обоснована избирательная установка туннелированных катетеров больным, нуждающимся в длительной медицинской помощи методами диализа.
Klouche K., Amigues L., Deleuze S., et al. Complications, effects on dialysis dose, and survival of tunneled femoral dialysis catheters in acute renal failure. Am J Kidney Dis 2007;49:99–108.
Oliver MJ, Edwards LJ, Treleaven DJ, et al. Randomized study of temporary hemodialysis catheters. Int J Artif Organs 2002;25:40–44.
Parienti J.J., Megarbane B., Fischer M.O., et al. Catheter dysfunction and dialysis performance according to vascular access among 736 critically ill adults requiring renal replacement therapy: a randomized controlled study. Crit Care Med 2010;38:1118–1125.
В России данных об использовании превалентными и инцидентными пациентами катетера в качестве сосудистого доступа нет. Всего за 2015 г. установлено 7978 ЦВК, то есть на каждого пролеченного пациента установлено в среднем 0,33 ЦВК, что не отличается от показателя 2013 г. и несколько меньше, чем в 2011 г. Анализ динамики показателя соотношения количества операций по формированию первичного сосудистого доступа к числу установленных ЦВК (количество операций по формированию АВФ/количество установленных ЦВК) на протяжении 2010–2015 гг. не позволяет говорить о какой-либо устойчивой тенденции, тем не менее складывается впечатление об уменьшении этого соотношения в 2015 г. (1,16 в 2015 г. и 0,88 в 2010 г.), что можно оценить как положительный тренд.
Томилина Н.А., Андрусев А.М., Перегудова Н.Г. и соавт. Заместительная терапия терминальной хронической почечной недостаточности в Российской Федерации в 2010–2015 гг. Отчет по данным Общероссийского регистра заместительной почечной терапии Российского диализного общества, Часть первая «Нефрология и диализ». 2017. 19(4 –Приложение): 1–95. Doi: 10.28996/1680-4422-2017-4suppl-1-95/
С 1997 по 2008 г. число пациентов, получавших лечение методами ПД, выросло по всему миру в 2,5 раза за счет превалентных пациентов развивающихся стран и составляет 1 % населения диализа. За 12 лет в развивающихся странах число больных, получавших лечение методами ПД, увеличилось и составило 24,9 на 1 млн населения и в развитых странах – 21,8 на 1 млн населения.
Arsh K. Jain, Global Trends in Rates of Peritoneal Dialysis. JASN23:533-544,2012.
В России в 2015 г. общее число ПД-больных к концу 2015 г. составило 2336 (15,9 больн./млн населения), или 5,3% от всех методов заместительной терапии почек. Сведения о формировании перитонеального доступа в 2015 г. были представлены 66 отделениями/центрами (59,4% от общего числа диализных центров, применявших ПД). В этих отделениях на конец года лечились ПД 1272 больных (54,5% от общего числа ПД-больных), и впервые в течение 2015 г. начали лечение ПД 407 пациентов (61,6% от общего количества «новых» ПД в целом по стране). За 2015 г. в них было имплантировано 626 катетеров, из которых 445 (71%) – хирургическое вмешательство и 183 (29%) – лапароскопическим методом. При этом в 56 (86,4%) из этих 66 отделений перитонеальный доступ формировался специально выделенным хирургом, в 11 (16,7%) – это выполнялось дежурными хирургами общей хирургической службы и в 2 (3%) – врачом-нефрологом.
Томилина Н.А., Андрусев А.М., Перегудова Н.Г. и соавт. Заместительная терапия терминальной хронической почечной недостаточности в Российской Федерации в 2010–2015 гг. Отчет по данным Общероссийского регистра заместительной почечной терапии Российского диализного общества. Часть первая «Нефрология и диализ». 2017. 19(4 – Приложение): 1–95. Doi: 10.28996/1680-4422-2017-4suppl-1-95.
КЛАССИФИКАЦИЯ
Доступ для диализа. Схема № 1
1. Доступ для экстракорпорального диализа:
a. Сосудистый доступ
i. Артериовенозный доступ
1. Артериовенозная фистула
2. Артериовенозный трансплантат:
a. Биологичекий
b. Протез
ii. Центральный венозный катетер:
1. Нетуннелированный катетер, безманжеточный
2. Туннелированный катетер
2. Доступ для перитонеального диализа:
a. Катетер для перитонеального диализа
Jan Tordoir, Bernard Canaud, Patrick Haage, Klaus Konner, Ali Basci, Denis Fouque, Jeroen Kooman, Alejandro Martin-Malo, Luciano Pedrini, Francesco Pizzarelli, James Tattersall, Marianne Vennegoor, Christoph Wanner, Piet ter Wee, Raymond Vanholder; EBPG on Vascular Access Nephrol Dial Transplant (2007) 22 [Suppl 2]: ii88–ii117. Doi:10.1093/ndt/gfm021
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55: 757–818
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232
Maurizio Gallieni et al. Clinical practice guideline on peri- and postoperative care of arteriovenous fistulas and grafts for haemodialysis in adults ERBP Guideline Development Group on Vascular Access Nephrol Dial Transplant (2019) 34: ii1–ii42. Doi: 10.1093/ndt/gfz072
Артериовенозный доступ для диализа
1. Направление пациента
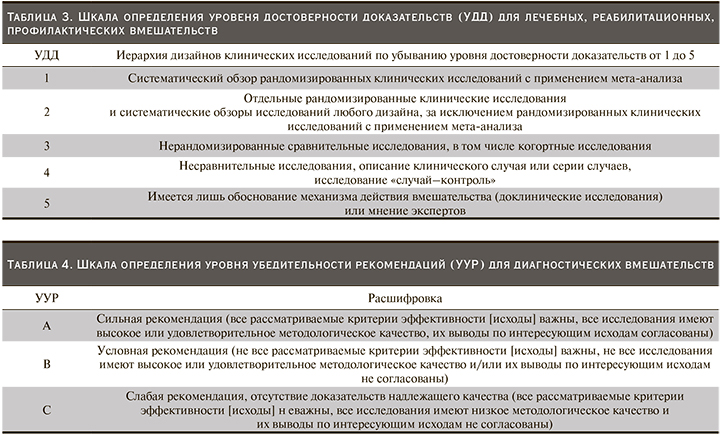
1.1. Мы предполагаем, что сохранение периферических вен предплечья – значимая часть обучения и образования взрослых пациентов при любой стадии ХБП, которым может потребоваться оказание медицинской помощи методами диализа независимо от выбора метода лечения.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций С
Jungers P, Massy ZA, Nguyen-Khoa T et al. Longer duration of predialysis nephrological care is associated with improved longterm survival of dialysis patients. Nephrol Dial Transplant 2001; 16: 2357–2364
Ravani P, Marcelli D, Malberti F. Vascular access surgery managed by renal physicians: the choice of native arteriovenous fistulas for hemodialysis. Am J Kidney Dis 2002; 40: 1264–1276
1.2. Предполагаем, что каждый взрослый пациент при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа, должен начать диализ с функционирующим сосудистым доступом.
Комментарии. В целях сохранения будущих вариантов сосудистого доступа медицинские работники должны избегать венепункции пациентам без необходимости при любой стадии ХБП, так как периферические вены верхней конечности могут быть использованы для его создания.
Уровень достоверности доказательств III, уровень убедительности рекомендаций В
European Best Practice Guidelines Expert Group on Hemodialysis, European Renal Association. Section I. Measurement of renal function, when to refer and when to start dialysis. Nephrol Dial Transplant 2002; 17 [Suppl 7]: 7–15
Allon M, Ornt DB, Schwab SJ et al. Factors associated with the prevalence of arteriovenous fistulas in hemodialysis patients in the HEMO study. Hemodialysis (HEMO) Study Group. Kidney Int 2000; 58: 2178–2185
Ortega T, Ortega F, Diaz-Corte C, Rebollo P, Ma Baltar J, Alvarez-Grande J. The timely construction of arteriovenous fistulae: a key to reducing morbidity and mortality and to improving cost management. Nephrol Dial Transplant 2005; 20: 598–603.
1.3. Предполагаем, что каждый потенциальный взрослый пациент ХБП-4 при достижении скорости клубочковой фильтрации менее 30 мл/мин/1,73 м2, которому показана медицинская помощь методами гемодиализа, в идеале должен быть направлен к нефрологу и/или хирургу для подготовки доступа к диализу или ранее в случае быстропрогрессирующей нефропатии, или конкретного клинического состояния, таких как сахарный диабет или тяжелые заболевания периферических сосудов.
Комментарии. Планирование доступа должно начинаться при ХБП-4. Своевременное направление пациента для создания АВ-доступа приводит к хорошо функционирующему АВ-доступу, замедлению снижения СКФ. Позднее направление к большей вероятности несозревания и необходимости ЦВК, последнее приводит к ухудшению долгосрочной проходимости и связано с большим риском окончательного отказа АВ-доступа. Сроки формирования сосудистого доступа определяется темпом снижения функции почек, сопутствующими заболеваниями и хирургическим вмешательством Знания и опыт хирурга в создании АВ-доступа имеют важное преимущество.
Уровень достоверности доказательств III, уровень убедительности рекомендаций В
Avorn J, Winkelmayer WC, Bohn RL, Levin R, Glynn RJ, Levy E, et al. Delayed nephrologist referral and inadequate vascular access in patients with advanced chronic kidney failure. J Clin Epidemiol 2002;55:711–716. de Jager DJ, Voormolen N, Krediet RT, Dekker FW, Boeschoten EW, Grootendorst DC. Association between time of referral and survival in the first year of dialysis in diabetics and the elderly. Nephrol Dial Transplant 2011;26:652–658.
Hasegawa T, Bragg-Gresham JL, Yamazaki S, Fukuhara S, Akizawa T, Kleophas W, et al. Greater first-year survival on hemodialysis in facilities in which patients are provided earlier and more frequent pre-nephrology visits. Clin J Am Soc Nephrol CJASN 2009;4:595–602.
Jan Tordoir, Bernard Canaud, Patrick Haage, Klaus Konner, Ali Basci, Denis Fouque, Jeroen Kooman, Alejandro Martin-Malo, Luciano Pedrini, Francesco Pizzarelli, James Tattersall, Marianne Vennegoor, Christoph Wanner, Piet ter Wee, Raymond Vanholder; EBPG on Vascular Access Nephrol Dial Transplant (2007) 22 [Suppl 2]: ii88–ii117 Doi:10.1093/ndt/gfm021.
Ortega T, Ortega F, Diaz-Corte C, Rebollo P, Ma Baltar J, Alvarez-Grande J. The timely construction of arteriovenous fistulae: a key to reducing morbidity and mortality and to improving cost management. Nephrol Dial Transplant 2005;20:598–603.
Prischl FC, Kirchgatterer A, Brandstatter E, Wallner M, Baldinger C, Roithinger FX, et al. Parameters of prognostic relevance to the patency of vascular access in hemodialysis patients. J Am Soc Nephrol 1995;6:1613–1618.
Ravani P, Brunori G, Mandolfo S, Cancarini G, Imbasciati E, Marcelli D, et al. Cardiovascular comorbidity and late referral impact arteriovenous fistula survival: a prospective multicenter study. J Am Soc Nephrol 2004;15:204–209.
Roubicek C, Brunet P, Huiart L, Thirion X, Leonetti F, Dussol B, et al. Timing of nephrology referral: influence on mortality and morbidity. Am J Kidney Dis 2000;36:35–41.
Saran R, Elder SJ, Goodkin DA, Akiba T, Ethier J, Rayner HC, et al. Enhanced training in vascular access creation predicts arteriovenous fistula placement and patency in hemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study. Ann Surg 2008;247:885–891.
Sumida K, Molnar MZ, Potukuchi PK, Thomas F, Lu JL, Ravel VA, et al. Association between vascular access creation and deceleration of estimated glomerular filtration rate decline in late-stage chronic kidney disease patients transitioning to end-stage renal disease. Nephrol Dial Transplant 2017;32:1330–1337.
2. Предоперационный осмотр
2.1. Предполагаем, что клиническая оценка и неинвазивные инструментальные методы исследования артерий верхних конечностей и вены с двух сторон должны быть выполнены до формирования сосудистого доступа.
Уровень достоверности доказательств II, уровень убедительности рекомендаций А
Комментарии. Пациенты должны быть обследованы с жгутом до операции в теплой комнате, и предлагаемая локализация АВ-доступа должна быть отмечена (картирована) до операции. Клиническая оценка и неинвазивные инструментальные методы (УЗИ артерий верхних конечностей и вены) должны быть выполнены до создания сосудистого доступа.
Allon M, Lockhart ME, Lilly RZ. Effect of preoperative sonographic mapping on vascular access outcomes in hemodialysis patients. Kidney Int 2001;60:2013–2020.
Brimble KS, Rabbat ChG, Treleaven DJ, Ingram AJ. Utility of ultrasonographic venous assessment prior to forearm arteriovenous fistula creation. Clin Nephrol 2002;58:122–127.
Chiang WC, Lin SL, Tsai TJ, Hsieh BS. High resistive index of the radial artery is related to early primary radiocephalic hemodialysis fistula failure. Clin Nephrol 2001;56:236–240.
Dalman RL, Harris Jr, EJ, Victor BJ, Coogan SM. Transition to all-autogenous hemodialysis access: the role of preoperative vein mapping. Ann Vasc Surg 2002;16:624–630.
Ferring M, Claridge M, Smith SA, Wilmink T. Routine preoperative vascular ultrasound improves patency and use of arteriovenous fistulas for hemodialysis: a randomized trial. Clin J Am Soc Nephrol CJASN 2010;5:2236–2244.
Georgiadis GS, Charalampidis DG, Argyriou C, Georgakarakos EI,
Lazarides MK. The necessity for routine preoperative ultrasound mapping before arteriovenous fistula creation: a meta-analysis. Eur J Vasc Endovasc Surg 2015;49:600–605.
Lemson MS, Leunissen KM, Tordoir JH. Does pre-operative duplex examination improve patency rates of Brescia-Cimino fistulas? Nephrol Dial Transpl 1998;13: 60–1361.
Lockhart ME, Robbin ML, Allon M. Preoperative sonographic radial artery evaluation and correlation with subsequent radiocephalic fistula outcome. J Ultras Med 2004; 23:161–168.
Malovrh M. Native arteriovenous fistula: preoperative evaluation. Am J Kidney Dis 2002; 9:218–1225.
Malovrh M. Non-invasive evaluation of vessels by duplex sonography prior to construction of arteriovenous fistulas for haemodialysis. Nephrol Dial Transpl 1998;13:125–129.
Mihmanli I, Besirli K, Kurugoglu S, Atakir K, Haider S, Ogut G, et al. Cephalic vein and hemodialysis fistula: surgeon’s observation versus color Doppler ultrasonographic findings. J Ultrasound Med 2001;20:217–222.
Patel ST, Hughes J, Mills Sr, JL. Failure of arteriovenous fistula maturation: an unintended consequence of exceeding dialysis outcome quality initiative guidelines for hemodialysis access. J Vasc Surg 2003;38:439–445.
Robbin ML, Gallichio MH, Deierhoi MH, Young CJ, Weber TM, Allon M. US vascular mapping before hemodialysis access placement. Radiology 2000;217:83–88.
Rooijens PPGM, Tordoir JHM, Stijnen T, Burgmans JPJ, Smet de AAEA, Yo TI. Radiocephalic wrist arteriovenous fistula for hemodialysis: meta-analysis indicates a high primary failure rate. Eur J Vasc Endovasc Surg 2004;28:571–680.
Rus RR, Ponikvar R, Kenda RB, Buturovic-Ponikvar J. Effect of local physical training on the forearm arteries and veins in patients with end-stage renal disease. Blood Purif 2003;21(6):389–394.
Lomonte C, Basile C. Preoperative assessment and planning of haemodialysis vascular access. Clin Kidney J 2015;8:278–281.
Schuman E, Standage BA, Ragsdale JW, Hein P. Achieving vascular access success in the quality outcomes era. Am J Surg 2004;187:585–589.
Silva Jr, MB, Hobson RW, Pappas PJ et al. A strategy for increasing use of autogenous hemodialysis access procedures: impact of preoperative noninvasive evaluation. J Vasc Surg 1998;27:302–307.
Vassalotti JA, Falk A, Cohl ED, Uribarri J, Teodorescu V. Obese and non-obese hemodialysis patients have a similar prevalence of functioning arteriovenous fistula using preoperative vein mapping. Clin Nephrol 2002;58:211–214.
Wong V, Ward R, Taylor J, Selvakumar S, How TV, Bakran A. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur J Vasc Endovasc Surg 1996;12:207–213.
2.2. Предполагаем, что исследование центральных вен показано пациентам при состояниях при ХБП-5, если в анамнезе присутствуют случаи использования центральных венозных катетеров для лечения.
Комментарии. Исследование центральных вен необходимо выполнять пациентам с анамнезом катетеризации, если восстановление функции почек маловероятно, так как имеет значительные долгосрочные отрицательные последствия.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций С
Geoffroy O, Tassart M, Le Blanche AF et al. Upper extremity digital subtraction venography with gadoterate meglumine before fistula creation for hemodialysis. Kidney Int 2001;59:1491–1497.
Menegazzo D, Laissy JP, Durrbach A et al. Hemodialysis access fistula creation: preoperative assessment with MR venography and comparison with conventional venography. Radiology 1998;209:723–728.
Paksoy Y, Gormus N, Tercan MA. Three-dimensional contrastenhanced magnetic resonance angiography (3-D CE-MRA) in the evaluation of hemodialysis access complications, and the condition of central veins in patients who are candidates for hemodialysis access. J Nephrol 2004;17:57–65.
Ascher E, Gade P, Hingorani A et al. Changes in the practice of angioaccess surgery: impact of dialysis outcome and quality initiative recommendations. J Vasc Surg 2000 (Jan);31(1 pt 1):84–92.
3. Концепция создания сосудистого доступа
3.1.Предполагаем, что сосудистый доступ должен обеспечивать достаточный кровоток для достижения адекватной дозы гемодиализа.
Уровень доказательности II
Hodges TC, Fillinger MF, Zwolak RM, Walsh DB, Bech F, Cronenwett JL. Longitudinal comparison of dialysis access methods: risk factors for failure. J Vascular Surg 1997;26:1009–1019.
Ifudu O, Mayers JD, Matthew JJ, Fowler A, Friedman EA. Haemodialysis dose is independent of type of surgically-created vascular access. Nephrol Dial Transpl 1998;13:2311–2316.
Cook JW, Schuman ES, Standage BA, Hein P. Patency and flow characteristics using stapled vascular anastomoses in dialysis grafts. Am J Surg 2001;181:24–27.
Lin SL, Huang CH, Chen HS, Hsu WA, Yen CJ, Yen TS. Effects of age and diabetes on blood flow rate and primary outcome of newly created hemodialysis arteriovenous fistulas. Am J Nephrol 1998;18:96–100.
3.2. Рекомендуем отдавать предпочтение аутогенной артериовенозной фистуле в качестве предпочтительного сосудистого доступа для начала лечения методами экстракорпорального диализа взрослых пациентов при состояниях при ХБП-5, артериовенозным трансплантатам следует отдавать предпочтение перед туннелированными центральными венозными катетерами для диализа.
Уровень достоверности доказательств II, уровень убедительности рекомендаций А
Комментарии. Индивидуальный выбор оптимального сосудистого доступа к диализу и определение сроков создания доступа зависят от наличия множество факторов, которые могут варьироваться в широких пределах для каждого пациента, включая демографию, сопутствующие заболевания, анатомию и личные предпочтения; часто решение о типе доступа зависит от состояния пациента, желаемого качества жизни и жизненных целей. Индивидуальный подход к созданию доступа с учетом интересов пациента играет важную роль в улучшении удовлетворенности пациентов и клинические результатов.
Allon M, Ornt DB, Schwab SJ et al. Factors associated with the prevalence of arteriovenous fistulas in hemodialysis patients in the HEMO study. Hemodialysis (HEMO) Study Group. Kidney Int 2000; 58:2178–218.5.
Antonious GA, Lazarides MK, Georgiadis GS, et al. Lower-extremity arteriovenous access for haemodialysis: a systematic review. Eur J Vasc Endovasc Surg. 2009;38:365–372.
Astor BC, Eustace JA, Powe NR, Klag MJ, Fink NE, Coresh J; CHOICE Study: Type of vascular access and survival among incident hemodialysis patients: The Choices for Healthy Outcomes in Caring for ESRD (CHOICE) Study. J Am Soc Nephrol 16:1449–1455, 2005.
Bello AK, Thadhani R, Hemmelgarn B, Klarenbach S, Gill J, Chan C, et al. Design and implementation of the Canadian kidney disease cohort study (CKDCS): a prospective observational study of incident hemodialysis patients. BMC Nephrol. 2011;12:10.
Canaud B, Tong L, Tentori F, et al. Clinical practices and outcomes in elderly hemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin J Am Soc Nephrol. 2011;6(7):1651–1662.
Centers for M, Medicaid Services HHS. Medicare Program; end stage renal disease prospective Payment system, Payment for renal dialysis Services Furnished to Individuals with Acute kidney Injury, and end-stage renal disease Quality Incentive Program. Final rule. Fed Regist. 2017;82(210):50738–50797.
Chan MR, Sanchez RJ, Young HN, et al. Vascular access outcomes in the elderly hemodialysis population: a USRDS study. Semin Dial. 2007;20:606–610.
Chertow GM, Levin NW, Beck GJ, et al. In-center hemodialysis six times per week versus three times per week. N Engl J Med. 2010;363:2287–-2300.
Jindal K, Chan CT, Deziel C et al. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. Chapter 4: vascular access. J Am Soc Nephrol 2006;17(Suppl 1):S16–S23
Lee T, Mokrzycki M, Moist L, Maya I, Vazquez M, Lok CE; North American Vascular Access Consortium: Standardized definitions for hemodialysis vascular access. Semin Dial 24:515–524,2011.
Manns B, Tonelli M, Yilmaz S, Lee H, Laupland K, Klarenbach S, Radkevich V, Murphy B: Establishment and maintenance of vascular access in incident hemodialysis patients: A prospective cost analysis. J Am Soc Nephrol 16:201–209, 2005.
Mendelssohn DC, Ethier J, Elder SJ, et al. Haemodialysis vascular access problems in Canada: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS II). Nephrol Dial Transplant. 2006;21:721–728.
Murad MH, Elamin MB, Sidawy AN, Malaga G, Rizvi AZ, Flynn DN, et al. Autogenous versus prosthetic vascular access for hemodialysis: a systematic review and meta-analysis. J Vasc Surg 2008;48:34S-47S.
National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for 2006 updates: hemo‐dialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis. 2006;48(Suppl 1):S1–S322.
Ng LJ, Chen F, Pisoni RL, Krishnan M, Mapes D, Keen M, et al. Hospitalization risks related to vascular access type among incident US hemodialysis patients. Nephrol Dial Transplant 2011;26:3659–3666.
Nguyen DB, Shugart A, Lines C, et al. National Healthcare safety Network (NHSN) dialysis event surveillance report for 2014. Clin J Am Soc Nephrol: CJASN. 2017;12(7):1139–1146.
Noordzij M, Jager KJ, van der Veer SN, et al. Use of vascular access for haemodialysis in Europe: a report from the ERA-EDTA Registry. Nephrol Dial Transplant. 2014;29:1956–1964.
Pisoni RL, Young EW, Dykstra DM et al. Vascular access use in Europe and the United States: results from the DOPPS. Kidney Int 2002; 61:305–316.
Pisoni RL, Zepel L, Fluck R, Lok CE, KawanishiH, Su¨ leymanlarG, Wasse H, Tentori F, Zee J, Li Y, Schaubel D, Burke S, Robinson B: International differences in the location and use of arteriovenous accesses created for hemodialysis: Results from the Dialysis Outcomes and Practice patterns study (DOPPS). Am J Kidney Dis 71:469–478,2018.
Pisoni RL, Zepel L, Port FK, et al. Trends in US vascular access use, patient preferences, and related practices: an update from the US DOPPS Practice Monitor with international comparisons. Am J Kidney Dis. 2015;65:905–915.
Polkinghorne K, Dent H, Gulyani A et al, Haemodialysis in ANZDATA Thirty Fourth Annual Report. 2011, Australia and New Zealand Dialysis and Transplant Registry: Adelaide, South Australia. Р. 5–25, 5–31.
Polkinghorne KR, Chin GK, MacGinley RJ, et al. KHA-CARI guideline: vascular access—central venous catheters, arteriovenous fistulae, and arteriovenous grafts. Nephrology. 2013;18:701–705.
Polkinghorne KR, McDonald SP, Atkins RC, Kerr PG. Epidemiology of vascular access in the Australian hemodialysis population. Kidney Int 2003;64:1893–1902.
Polkinghorne KR, McDonald SP, Marshall MR, Atkins RC, Kerr PG. Vascular access practice patterns in the New Zealand hemodialysis population. Am J Kidney Dis 2004;43:696–704.
PROSPERO: International prospective register of systematic reviews: Vascular access in intensive hemodialysis: a systematic review and meta-analysis. http://www.crd.york.ac.uk/ PROSPERO/display_record.asp?ID_CRD42012001967. Accessed May 21, 2013.
Quinn R, Ravani P, ACCESS HD Investigators. ACCESS HD pilot: a randomised feasibility trial comparing catheters with fistulas in elderly patients starting haemodialysis. BMJ Open. 2016;6:-013081.
Ravani P, Palmer SC, Oliver MJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol. 2013; 24:465–473.
Rayner HC, Pisoni RL. The increasing use of hemodialysis catheters: evidence from the DOPPS on its significance and ways to reverse it. Semin Dial. 2010;23:6.
Rodriguez JA, Lopez J, Cleries M, Vela E. Vascular access for haemodialysis – an epidemiological study of the Catalan Renal Registry. Nephrol Dial Transpl 1999;14:1651–1657.
Saran R, Robinson B, Abbott KC, et al. US renal data system 2017 annual data report: Epidemiology of kidney disease in the United States. Am J Kidney Dis. 2018;71(3):A7.
Sequeira A, Naljayan M, Vachharajani TJ. Vascular access guidelines: summary, rationale, and controversies. Tech Vasc Interv Radiol. 2017;20:2–8.
Thomas B, Wulf S, Bikbov B, et al. Maintenance dialysis throughout the world in years 1990 and 2010. J Am Soc Nephrol. 2015;26:2621–2633.
United States Renal Data Systems. (2016). Annual Data Report. Bethesda, MD: The National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. https://www. usrds.org. Accessed 26 January 2019.
Viecelli AK, Tong A, O’Lone E, et al. Report of the Standardised Outcomes in Nephrology-Hemodialysis (SONG-HD) Consensus Workshop on Establishing a Core Outcome Measure for Hemodialysis Vascular Access. Am J Kidney Dis. 2018;71:690–700.
Wish JB. Vascular access for dialysis in the United States: progress, hurdles, controversies, and the future. Semin Dial. 2010;23:614–618.
Young EW, Dykstra DM, Goodkin DA, Mapes DL, Wolfe RA, Held PJ. Hemodialysis vascular access preferences and outcomes in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int 2002; 61: 2266–2271.
Сrosswell A, Brain MJ, Roodenburg O. Vascular access site influences circuit life in continuous renal replacement therapy. Crit Care Resusc J Australas Acad Crit Care Med 2014;16:127–130.
3.3. Полагаем, что недостаточно данных о преимуществе анастомоза «конец вены в бок артерии» перед анастомозом «бок вены в бок артерии» при формировании артериовенозной фистулы у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций С
Bashar K, Medani M, Bashar H et al. End-to-side versus side-to-side anastomosis in upper limb arteriovenous fistula for dialysis access: a systematic review and a meta-analysis. Ann Vasc Surg 2018;47:43–53.
Wedgwood KR, Wiggins PA, Guillou PJ. A prospective study of end-toside vs. side-to-side arteriovenous fistulas for haemodialysis. Br J Surg 1984;7:640–642.
Mozaffar M, Fallah M, Lotfollahzadeh S et al. Comparison of efficacy of side to side versus end to side arteriovenous fistulae formation in chronic renal failure as a permanent hemodialysis access. Nephro-Urol Monthly 2013;5:827–830.
Khan MW, Khan MM, Qadir I et al. Comparative study of efficacy of endto- side with side-to-side arteriovenous fistula in patients on hemodialysis. Pakistan JMed Health Sci 2015;9:235–238.
Schild AF, Raines J. Preliminary prospective randomized experience with vascular clips in the creation of arteriovenous fistulae for hemodialysis. Am J Surg 1999;178:33–37.
Walker S. U Clips for arteriovenous anastomosis: a pilot, randomized study. ANZ J Surg 2012;82:630–632.
Zeebregts CJ, van den Dungen JJ, van Det RJ et al. Randomized clinical trial of continuous sutures or non-penetrating clips for radiocephalic arteriovenous fistula. Br J Surg 2004;91:1438–1442.
Beigi AA, Masoudpour H, Alavi M. The effect of ligation of the distal vein in snuff-box arteriovenous fistula. Saudi J Kidney Dis Transpl 2009;20:1110–1114.
Laskar M, Cornu E, Leman A et al. Anastomosis of small caliber vessels. Comparison between continuous or interrupted suture. Presse Med 1988;17:1152–1153.
Kakkos SK, Tsolakis IA, Papadoulas SI et al. Randomized controlled trial comparing primary and staged basilic vein transposition. Front Surg 2015;2:14.
Veroux P, Giaquinta A, Tallarita T et al. Primary balloon angioplasty of small (<2 mm) cephalic veins improves primary patency of arteriovenous fistulae and decreases reintervention rates. J Vasc Surg 2013;57:131–136.
3.4. Предлагаем использовать верхнюю конечность как предпочтительное место доступа к формированию АВ-фистулы, и она должна располагаться как можно дистальнее.
Уровень достоверности доказательств II, уровень убедительности рекомендаций А
Артериовенозные фистулы
Комментарии. АВ-фистула (А.radialis – V. Cephalica) рекомендуется в качестве предпочтительного сосудистого доступа. При адекватном состоянии сосудов недоминантную конечность следует рассматривать как предпочтительное место для формирования АВ-фистулы. Необходимо рассматривать альтернативную локализацию АВ-доступа у взрослых пациентов, если при ультразвуковом исследовании внутренний диаметр лучевой артерии меньше 2,0 мм и/или диаметр подкожной латеральной вены (V. Cephalica) меньше 2,0 мм. АВ-доступ на нижней конечности следует рассматривать, только когда доступ к верхней конечности невозможен. Если используется постоянный ЦВК или кардиостимулятор, АВ-доступ должен быть сформирован на противоположной руке из-за риска центрального венозного стеноза и снижения проходимости АВ-доступа.
Antoniou GA, Lazarides MK, Georgiadis GS, Sfyroeras GS, Nikolopoulos ES, Giannoukas AD. Lower-extremity arteriovenous access for haemodialysis: a systematic review. Eur J Vasc Endovasc Surg 2009;38:365–372.
Bourquelot P, Rawa M, Van Laere O, Franco G. Long-term results of femoral vein transposition for autogenous arteriovenous hemodialysis access. J Vasc Surg 2012;56:440–445.
D’Ayala M, Smith RM, Martone C, Briggs W, Deitch JS, Wise L. The effect of systemic anticoagulation in patients undergoing angioaccess surgery. Ann Vasc Surg 2008;22:11e5.
Fitzgerald JT, Schanzer A, Chin AI, McVicar JP, Perez RV, Troppmann C. Outcomes of upper arm arteriovenous fistulas for maintenance hemodialysis access. Arch Surg 2004; 139: 201–208.
Gradman WS, Laub J, Cohen W. Femoral vein transposition for arteriovenous hemodialysis access: improved patient selection and intraoperative measures reduce postoperative ischemia. J Vasc Surg 2005;41:279–284.
Keuter XH, De Smet AA, Kessels AG, van der Sande FM, Welten RJ, Tordoir JH. A randomized multicenter study of the outcome of brachial-basilic arteriovenous fistula and prosthetic brachial-antecubital forearm loop as vascular access for hemodialysis. J Vasc Surg 2008;47:395–401.
Kim YO, Song HC, Yoon SA et al. Preexisting intimal hyperplasia of radial artery is associated with early failure of radiocephalic arteriovenous fistula in hemodialysis patients. Am J Kidney Dis 2003;41:422–428.
Kordzadeh A, Chung J, Panayiotopoulos YP. Cephalic vein and radial artery diameter in formation of radiocephalic arteriovenous fistula: a systematic review. J Vasc Access 2015;16:506–511.
Morosetti M, Cipriani S, Dominijanni S, Pisani G, Frattarelli D, Bruno F. Basilic vein transposition versus biosynthetic prosthesis as vascular access for hemodialysis. J Vasc Surg 2011;54:1713–1719.
Murad MH, Elamin MB, Sidawy AN, Malaga G, Rizvi AZ, Flynn DN, et al. Autogenous versus prosthetic vascular access for hemodialysis: a systematic review and meta-analysis. J Vasc Surg 2008;48:34S–47S.
Ng LJ, Chen F, Pisoni RL, Krishnan M, Mapes D, Keen M, et al. Hospitalization risks related to vascular access type among incident US hemodialysis patients. Nephrol Dial Transplant 2011;26:3659–3666.
Oliver MJ, McCann RL, Indridason OS, Butterly DW, Schwab SJ. Comparison of transposed brachiobasilic fistulas to upper arm grafts and brachiocephalic fistulas. Kidney Int 2001;60:1532–1539.
Rooijens PPGM, Tordoir JHM, Stijnen T, Burgmans JPJ, Smet de AAEA, Yo TI. Radiocephalic wrist arteriovenous fistula for hemodialysis: meta-analysis indicates a high primary failure rate. Eur J Vasc Endovasc Surg 2004;28:571–680.
White G, Wilson S. Planning and patient assessment for vascular access surgery. In: Wilson S, editor. Vascular access principles and practice. 4th ed. St. Louis: Mosby; 2002. Р. 7–13.
Wong V, Ward R, Taylor J, Selvakumar S, How TV, Bakran A. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur J Vasc Endovasc Surg 1996;12:207–213.
Yoo DW, Yoon M, Jun HJ. Successful access rate and risk factor of vascular access surgery in arm for dialysis. Vasc Spec Int 2014;30:33–37.
Артериовенозные трансплантаты
Комментарии. При недоступности латеральной подкожной вены руки V. Cephalica предпочтение следует отдавать АВ-трансплантату из-за лучшей проходимости и низкого риска инфицирования, чем транспозиции медиальной подкожной вены руки (V. Basilica) для АВ-фистулы.
Keuter XH, De Smet AA, Kessels AG, van der Sande FM, Welten RJ, Tordoir JH. A randomized multicenter study of the outcome of brachial-basilic arteriovenous fistula and prosthetic brachial-antecubital forearm loop as vascular access for hemodialysis. J Vasc Surg 2008;47:395–401.
Morosetti M, Cipriani S, Dominijanni S, Pisani G, Frattarelli D, Bruno F. Basilic vein transposition versus biosynthetic prosthesis as vascular access for hemodialysis. J Vasc Surg 2011;54:1713–1719.
Комментарии. При необходимости формирования АВ-доступа на нижних конечностях транспозиция бедренной вены более предподчтительна, чем АВ-трансплантат. Antoniou GA, Lazarides MK, Georgiadis GS, Sfyroeras GS, Nikolopoulos ES, Giannoukas AD. Lower-extremity arteriovenous access for haemodialysis: a systematic review. Eur J Vasc Endovasc Surg 2009;38:365–372.
Hazinedaroglu SM, Tuzuner A, Ayli D, Demirer S, Duman N, Yerdel MA. Femoral vein transposition versus femoral loop grafts for hemodialysis: a prospective evaluation. Transplant Proc 2004;36:65–67.
Комментарии. При невозможности формирования АВ-фистулы и при наличии инфекции следует отдавать предпочтение скорее биологическому, чем синтетическому сосудистому трансплантату.
Berardinelli L. Grafts and graft materials as vascular substitutes for haemodialysis access construction. Eur J Vasc Endovasc Surg 2006;32:203–211.
Kennealey PT, Elias N, Hertl M, Ko DS, Saidi RF, Markmann JF, et al. A prospective, randomized comparison of bovine carotid artery and expanded polytetrafluoroethylene for permanent hemodialysis vascular access. J Vasc Surg 2011;53:1640–1648.
Tahami VB, Hakki H, Reber PU, Widmer MK, Kniemeyer HW. Polytetrafluoroethylene and bovine mesenterial vein grafts for hemodialysis access: a comparative study. J Vasc Access 2007;8:17–20.
Комментарии. Мы предлагаем взрослым пациентам использовать артериовенозный трансплантат, «предназначенный для ранней канюляции», в качестве АВ-доступа при затруднительном формировании центрального венозного доступа.
Chemla ES, Nelson S, Morsy M. Early cannulation grafts in straight axillo-axillary angioaccesses avoid central catheter insertions. Semin Dial 2011;24:456–459.
Артериовенозный доступ
Комментарии. Когда стандартные локализации сосудистого доступа на верхней конечности исчерпаны, следует рассмотреть сложные процедуры доступа в зависимости от наличия подходящих сосудов.
4. Периоперационные вмешательства при формировании артериовенозного доступа
4.1. Предлагаем использовать при формировании артериовенозной фистулы у взрослых пациентов регионарную анестезию вместо местной.
Уровень достоверности доказательств II, уровень убедительности рекомендаций В
Комментарии. Регионарная анестезия – предпочтительный вариант при операциях по формированию сосудистого доступа по сравнению с местной анестезией в связи с более высокой вероятностью улучшения проходимости доступа.
Aitken E, Jackson A, Kearns R et al. Effect of regional versus local anaesthesia on outcome after arteriovenous fistula creation: a randomised controlled trial. Lancet 2016;388:1067–1074.
Hingorani AP, Ascher E, Gupta P, Alam S, Marks N, Schutzer RW, et al. Regional anesthesia: preferred technique for venodilatation in the creation of upper extremity arteriovenous fistulae. Vascular 2006;14:23–26.
Ismail A, Abushouk AI, Bekhet AH et al. Regional versus local anesthesia for arteriovenous fistula creation in end-stage renal disease: a systematic review and meta-analysis. J Vasc Access 2017;18:177–184.
Lo Monte AI, Damiano G, Mularo A, Palumbo VD, Alessi R, Gioviale MC, et al. Comparison between local and regional anesthesia in arteriovenous fistula creation. J Vasc Access 2011;12:331–335.
Malinzak EB, Gan TJ. Regional anesthesia for vascular access surgery. Anesth Analg 2009;109:976–980.
Meena S, Arya V, Sen I et al. Ultrasound-guided supraclavicular brachial plexus anaesthesia improves arteriovenous fistula flow characteristics in end-stage renal disease patients. South Afr J Anaesth Analg 2015;21:12–15.
Laskowski IA, Muhs B, Rockman CR, Adelman MA, Ranson M, Cayne NS, et al. Regional nerve block allows for optimization of planning in the creation of arteriovenous access for hemodialysis by improving superficial venous dilatation. Ann Vasc Surg 2007;21:730e3.
Reynolds TS, Kim KM, Dukkipati R, Nguyen TH, Julka I, Kakazu C, et al. Pre-operative regional block anesthesia enhances operative strategy for arteriovenous fistula creation. J Vasc Access 2011;12:336–340.
Sahin L, Gul R, Mizrak A et al. Ultrasound-guided infraclavicular brachial plexus block enhances postoperative blood flow in arteriovenous fistulas. J Vasc Surg 2011;54:749–753.
Sahin L, Gul R, Mizrak A, Deniz H, Sahin M, Koruk S, et al. Ultrasound-guided infraclavicular brachial plexus block enhances postoperative blood flow in arteriovenous fistulas. J Vasc Surg 2011;54:749–753.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Shoshiashvili V, Tataradze A, Beglarishvili L et al. Influence of type of anesthesia on hemodynamic parameters and outcome of dialysis arteriovenous fistula operations. GeorgianMed News 2015;249:20–27.
Thomsen M, Bengtsson M, Lassvik C et al. Adjuvant intravenous sympathetic block with guanethidine in construction of arteriovenous fistulas for blood access. Acta Chir Scand 1983;149:141–145.
Yildirim V, Doganci S, Yanarates O et al. Does preemptive stellate ganglion blockage increase the patency of radiocephalic arteriovenous fistula? Scand Cardiovasc J 2006;40:380–384.
4.2. Предлагаем использовать адекватную предоперационную гидратацию при создании АВ-доступа у взрослых пациентов.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций С
Malovrh M. Expansion of blood volume increases the primary patency rate of arteriovenous fistulas for hemodialysis in patients with critical arterial quality. Ther Apher Dial 2009;13:345–349.
4.3. Предлагаем назначать плановые операции, связанные с АВ-доступом, в день между процедурами гемодиализа, чтобы уменьшить воздействие препаратов на антикоагуляции, которые используются во время гемодиализа.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Padberg Jr FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg 2008;48:55S–80S.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
4.4. Мы рекомендуем проводить предоперационную профилактику антибиотиками перед установкой артериовенозного трансплантата взрослым пациентам при состояниях при ХБП-5.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. При выявлении MRSA рекомендуется назначение гликопептида парентерально.
Bennion R, Hiatt JR, Williams R et al. A randomized, prospective study of perioperative antimicrobial prophylaxis for vascular access surgery. J Cardiovasc Surg 1985;26:270–274.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Stewart AH, Eyers PS, Earnshaw JJ. Prevention of infection in peripheral arterial reconstruction: a systematic review and meta-analysis. J Vasc Surg 2007;46:148–155.
Zibari G, Gadallah M, Landreneau M et al. Preoperative vancomycin prophylaxis decreases incidence of postoperative hemodialysis vascular access infections. Am J Kidney Dis 1997;30:343–348.
4.5. Предлагаем проводить предоперационную профилактику антибиотиками перед обширными (сложными) оперативными вмешательствами по формированию артериовенозного доступа взрослым пациентам при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. Простые оперативные вмешательства по формированию артериовенозного доступа включают формирование нативной радиоцефальной или нативной брахиоцефальной артериовенозной фистулы.
National Institute for Health and Care Excellence. Surgical Site Infections: Prevention and Treatment. NICE Guideline CG74. https://www.nice.org. uk/guidance/cg74; London: National Institute for Health and Care Excellence.
4.6 Предполагаем, что не следует проводить предоперационную профилактику антибиотиками перед простым оперативным вмешательством по формированию артериовенозного доступа взрослым пациентам при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. Обширные (сложные) оперативные вмешательства по формированию артериовенозного доступа включают процедуры, не относящиеся к категории простых.
National Institute for Health and Care Excellence. Surgical Site Infections: Prevention and Treatment. NICE Guideline CG74. https://www.nice.org. uk/guidance/cg74; London: National Institute for Health and Care Excellence.
5. Медицинская помощь для созревания артериовенозной фистулы
5.1. Мы предлагаем назначение либо аспирина, либо тиклопидина, или клопидогрела взрослым пациентам при состояниях при ХБП-5 первые два месяца после формирования артериовенозной фистулы с единственной целью – обеспечения созревания АВ-фистулы. При этом должен соблюдаться баланс между желанием снизить риск тромбоза и непредсказуемым воздействием на созревание и риск кровотечения.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Необходимо применять индивидуальный подход к назначению антитромбоцитарных препаратов для предотвращения тромбоза нативных АВ-фистул.
Palmer SC, Di Micco L, Razavian M et al. Antiplatelet therapy to prevent hemodialysis vascular access failure: systematic review and meta-analysis. Am J Kidney Dis 2013;61:112–122.
Tanner NC, Da Silva A. Medical adjuvant treatment to increase patency of arteriovenous fistulae and grafts. Cochrane Database Syst Rev 2015;7:CD002786.
Palmer SC, Di Micco L, Razavian M et al. Antiplatelet agents for chronic kidney disease. Cochrane Database Syst Rev 2013;4 CD008834.
Andrassy K, Malluche H, Bornefeld H et al. Prevention of p.o. clotting of av. cimino fistulae with acetylsalicyl acid. Results of a prospective double blind study. KlinWochenschr 1974;52:348–349.
Abacilar AF, Atalay H, Dogan OF. Oral prostacycline analog and clopidogrel combination provides early maturation and long-term survival after arteriovenous fistula creation: a randomized controlled study. Indian J Nephrol 2015;25:136–142.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
5.2. Мы предполагаем, что любое решение о периоперационном назначении гепарина взрослым пациентам при состояниях при ХБП-5 при формировании артериовенозной фистулы должно соблюдать баланс между повышением проходимости артериовенозной фистулы через месяц после формирования и значимым ростом риска геморрагических осложнений.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Smith GE, Souroullos P, Cayton T et al. A systematic review and metaanalysis of systemic intraoperative anticoagulation during arteriovenousaccess formation for dialysis. J Vasc Access 2016;17:1–5.
Chen L, Ling YS, Lin CH et al. Combined use of heparin and anisodamine reduces the risk of early thrombosis in native arteriovenous fistula. Vascular 2013;21:369–374.
5.3. Предполагаем, что любое решение о применении длинноволновой инфракрасной терапии взрослым пациентам при состояниях при ХБП-5 в первые 3 месяца после формирования артериовенозной фистулы должно соблюдать баланс между снижением риска тромбоза и непредсказуемым воздействием на созревание и риск кровотечения.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Bashar K, Healy D, Browne LD et al. Role of far infra-red therapy in dialysis arterio-venous fistula maturation and survival: systematic review and meta-analysis. PLoS One 2014;9:e104931.
Wan Q, Yang S, Li L et al. Effects of far infrared therapy on arteriovenous fistulas in hemodialysis patients: a meta-analysis. Renal Failure 2017;39:613–622.
5.4. На текущий момент имеется недостаточное количество данных рандомизированных контролируемых исследований для рекомендации тикагрелора (ticagrelor), прасугрела (prasugrel), дипиридамола (dipyridamole), сулфинпиразона (sulphinpyrazone), варфарина (warfarin) или других пероральных антикоагулянтов, рыбьего жира, статинов, вонапанитазы (vonapanitase), глицерил-тринитрата (glyceryl trinitrate), ионофоретических инъекций шалфея многокорневищного (Salvia miltiorrhiza) или преднизолона для обеспечения созревания артериовенозной фистулы у взрослых при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Abacilar AF, Atalay H, Dogan OF. Oral prostacycline analog and clopidogrel combination provides early maturation and long-term survival after arteriovenous fistula creation: a randomized controlled study. Indian J Nephrol 2015;25:136–142.
Bleyer A, Kidd K, Wilson S et al. The effect of topically applied vonapanitase on fistula outcomes: results of the patency-1 trial. Am J Kidney Dis 2017;69:A2.
Crowther MA, Clase CM, Margetts PJ, Julian J, Lambert K, Sneath D, et al. Low-intensity warfarin is ineffective for the prevention of PTFE graft failure in patients on hemodialysis: a randomized controlled trial. J Am Soc Nephrol 2002;13:2331–2337.
Field M, McGrogan D, Marie Y et al. Randomized clinical trial of the use of glyceryl trinitrate patches to aid arteriovenous fistula maturation. Br J Surg 2016;103:1269–1275.
Irish AB, Viecelli AK, Hawley CM et al. Effect of fish oil supplementation and aspirin use on arteriovenous fistula failure in patients requiring hemodialysis. JAMA Intern Med 2017;177:184–193.
Rongrong W, Li D, Guangqing Z et al. The effects of iontophoretic injections of Salvia miltiorrhiza on the maturation of the arteriovenous fistula: a randomized controlled trial. Altern Ther Health Med 2016;22:18–22.
Saran R, Dykstra DM, Wolfe RA, Gillespie B, Held PJ, Young EW. Association between vascular access failure and the use of specific drugs: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2002;40:1255–1263.
Sharathkumar A, Hirschl R, Pipe S, Crandell C, Adams B, Lin JJ. Primary thromboprophylaxis with heparins for arteriovenous fistula failure in pediatric patients. J Vasc Access 2007;8:235–244.
Tanner NC, Da Silva A. Medical adjuvant treatment to increase patency of arteriovenous fistulae and grafts. Cochrane Database Syst Rev 2015;7:CD002786.
Viecelli AK, Irish AB, Polkinghorne KR et al. Omega-3 polyunsaturated fatty acid supplementation to prevent arteriovenous fistula and graft failure: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis 2018;72:50–61.
Voorzaat BM, van Schaik J, van der Bogt KEA et al. Improvement of radiocephalic fistula maturation: rationale and design of the Liposomal Prednisolone to Improve Hemodialysis Fistula Maturation (LIPMAT) study – a randomized controlled trial. J Vasc Access 2017;18:114–117.
Wasse H, Huang R, Long Q et al. Very high-dose cholecalciferol and arteriovenous fistula maturation in ESRD: a randomized, double-blind, placebo- controlled pilot study. J Vasc Access 2014;15:88–94.
Комментарии. Не прерывайте антитромбоцитарную монотерапию взрослых при формировании АВ-доступа.
Lewis SR, Pritchard MW, Schofield-Robinson OJ et al. Continuation versus discontinuation of antiplatelet therapy for bleeding and ischaemic events in adults undergoing non-cardiac surgery. Cochrane Database Syst Rev 2018;7:CD012584.
6. Вмешательства, направленные на созревание артериовенозной фистулы, выполняемые самостоятельно пациентом
6.1 Предполагаем, что стандартизированная программа упражнений, включающих таковые для кисти руки и руки, может способствовать скорейшему созреванию АВ-фистулы у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Desai S, Mitra A, Arkans E et al. Early application of an intermittent pneumatic compression device is safe and results in proximal arteriovenous fistula enlargement. J Vasc Access 2019;20:24–30.
Fontsere´ N, Mestres G, Yugueros X et al. Effect of a postoperative exercise program on arteriovenous fistula maturation: a randomized controlled trial. Hemodial Int 2016;20:306–314.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017; 37(Suppl 1):1–191.
Kong S, Lee KS, Kim J et al. The effect of two different hand exercises on grip strength, forearm circumference, and vascular maturation in patients who underwent arteriovenous fistula surgery. Ann Rehabil Med 2014;38:648–657.
Salimi F,Majd NG, MoradiMet al. Assessment of effects of upper extremity exercise with arm tourniquet on maturity of arteriovenous fistula in hemodialysis patients. J Vasc Access 2013;14 239–244.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Workgroup VA. Clinical practice guidelines for vascular access. Am J Kidney Dis 2006; 48(Suppl 1):S176–S247.
6.2. Существует недостаточно данных в пользу специфических комплексов упражнений или физических процедур для ускорения созревания АВ-фистулы у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. Более активное участие пациентов в подготовке к гемодиализу может способствовать улучшению навыков самопомощи и повышению грамотности пациентов, что может способствовать улучшению их самочувствия.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
7. Роль среднего медицинского персонала при оказании медицинского ухода за АВ-доступом
7.1. Предлагаем участвовать среднему медицинскому персоналу в сохранении периферических вен и мониторинге сосудистого доступа.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Комментарии. Каждый взрослый пациент при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа, должен пройти обучение потенциальным вариантам доступа и получить образование по сохранению сосудистого доступа. Предотвращение образования аневризмы ассоциируется с отсутствием нарушений в технике пункций доступа и является краеугольным камнем для сохранения артериовенозной фистулы.
Konner K. Venous preservation. Blood Purif 2002;19:115.
Hayes J. The role of nurses in maintenance of vascular access function. EDTNA/ERCA J 1998; XXIV:9–12.
Hartigan MF. Vascular access and nephrology nursing practice: existing views and rationales for change. Adv Renal Replacement Ther 1994;1:155–162.
7.2. Предлагаем проводить систематическое обучение и переподготовку медицинского персонала, участвующего в канюляции или в уходе за сосудистым доступом.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Комментарии. Образование медицинского персонала является решающими в успехе качества медицинской помощи. Для улучшения ухода и клинических результатов необходимо назначать одну или несколько медсестер, ответственных за сосудистый доступ.
Dwyer A, Shelton P, Brier M, Aronoff G. A vascular access coordinator improves the prevalent fistula rate. Semin Dial 2012;25:239–243.
Dinwiddie LC. Investing in the lifeline: the value of a vascular access coordinator. Nephrol News Issues 2003;17.49,52–53.
Leitch R, Ouwendyk M, Ferguson E et al. Nursing issues related to patient selection, vascular access, and education in quotidian hemodialysis. Am J Kidney Dis 2003;42 [Supp 1]:S56–S60.
Gelmez M, Akcaoglu T, Utkucu UЁ . Integrated education of nurses on vascular access for haemodialysis. EDTNA/ERCA J 2002; XXVIII:36–38.
Saran R, Dykstra DM, Pisoni RL et al. Timing of first cannulation and vascular access failure in haemodialysis: an analysis of practice patterns at dialysis facilities in the DOPPS. Nephrol Dial Transplant 2004;19:2334–2340.
Ravani P, Brunori G, Mandolfo S et al. Cardiovascular comorbidity and late referral impact arteriovenous fistula survival: a prospective multicenter study. J Am Soc Nephrol 2004;15:204–209.
Brunori G, Ravani P, Mandolfo S, Imbasciati E, Malberti F, Cancarini G. Fistula maturation: doesn’t time matter at all? Nephrol Dial Transplant 2005;20:684–687.
Basile C, Casucci F, Lomonte C. Timing of first cannulation of arteriovenous fistula: time matters, but there is also something else. Nephrol Dial Transplant 2005;20:1519–1520.
8. Наблюдение за созреванием артериовенозной фистулы
8.1. Предлагаем наблюдение на регулярной основе за созреванием артериовенозной фистулы, чтобы выполнять при необходимости упреждающие вмешательства.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Комментарии. Гемодиализ следует начинать при условии функционирования сосудистого доступа. Доступ должен обеспечивать достаточный кровоток для выполнения достижения адекватной дозы гемодиализа. Систематический уход, мониторинг, обследование используются для прогнозирования и предотвращения несостоятельности доступа. Перед использованием АВ-доступа до любой канюляции необходимо провести клиническую оценку и неинвазивное исследование при помощи инструментальных методов.
Astor BC, Eustace JA, Powe NR et al. Timing of nephrologist referral and arteriovenous access use: the CHOICE Study. Am J Kidney Dis 2001;38:494–501.
Astor BC, Eustace JA, Powe NR, Klag MJ, Fink NE, Coresh J. CHOICE Study. Type of vascular access and survival among incident hemodialysis patients: the Choices for Healthy Outcomes in Caring for ESRD (CHOICE) Study. J Am Soc Nephrol 2005;16:1449–1455.
Avorn J, Winkelmayer WC, Bohn RL et al. Delayed nephrologist referral and inadequate vascular access in patients with advanced chronic kidney failure. J Clin Epidemiol 2002;55:711–716.
Beathard GA, Arnold P, Jackson J, Litchfield T. Aggressive treatment of early fistula failure. Kidney Int 2003; 4:1487–1494.
Besarab A. Access Monitoring is worthwhile and valuable. Blood Purif 2006;24:77–89.
Besarab A. Preventing vascular access dysfunction: which policy to follow. Blood Purif 2002;20:26–35.
European Best Practice Guidelines Expert Group on Hemodialysis, European Renal Association. Section I. Measurement of renal function, when to refer and when to start dialysis. Nephrol Dial Transplant 2002; 17[Suppl 7]:7–15.
Gibson KD, Gillen DL, Caps MT, Kohler TR, Sherrard DJ, Stehman-Breen CO. Vascular access survival and incidence of revisions: a comparison of prosthetic grafts, simple autogenous fistulas, and venous transposition fistulas from the United States Renal Data System Dialysis Morbidity and Mortality Study. J Vasc Surg 2001;34:694–700.
Hingorani A, Ascher E, Kallakuri S, Greenberg S, Khanimov Y. Impact of reintervention for failing upper-extremity arteriovenous autogenous access for hemodialysis. J Vasc Surg 2001;34:1004–1009.
Kim YO, Yang CW, Yoon SA et al. Access blood flow as a predictor of early failures of native arteriovenous fistulas in hemodialysis patients. Am J Nephrol 2001;21:221–225.
May RE, Himmelfarb J, Yenicesu JM et al. Predictive measures of vascular access thrombosis: a prospective study. Kidney Int 1997;52:1656–1662.
McCarley P, Wingard RL, Shyr Y, Pettus W, Hakim RM, Ikizler TA. Vascular access blood flow monitoring reduces access morbidity and costs. Kidney Int 2001;60:1164–1172.
Sands JJ, Jabyac PA, Miranda CL, Kapsick BJ. Intervention based on monthly monitoring decreases hemodialysis access thrombosis. ASAIO J 1999;45:147–150.
Sands JJ. Vascular access monitoring improves outcomes. Blood Purif 2005:23:45–49.
Saran R, Dykstra DM, Wolfe RA, Gillespie B, Held PJ, Young EW. Dialysis Outcomes and Practice Patterns Study. Association between vascular access failure and the use of specific drugs: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis 2002;40:1255–1263.
Schwab SJ, Raymond JR, Saeed M, Newman GE, Dennis PA, Bollinger RR. Prevention of hemodialysis fistula thrombosis. Early detection of venous stenoses. Kidney Int 1989;36:707–711.
Sedlacek M, Teodorescu V, Falk A, Vassalotti JA, Uribarri J. Hemodialysis access placement with preoperative noninvasive vascular mapping: comparison between patients with and without diabetes. Am J Kidney Dis 2001;38:560–564.
Smits JH, Linden J van der, Hagen EC et al. Graft surveillance: venous pressure, access flow, or the combination? Kidney Int 2001;59:1551–1558.
Spergel LM, Holland JE, Fadem SZ, McAllister CJ, Peacock EJ. Static intra-pressure ratio does not correlate with access blood flow. Kidney Int 2004; 66:1512–1516.
Sullivan KL, Besarab A, Dorrell S, Moritz MJ. The relationship between dialysis graft pressure and stenosis. Invest Radiol 1992;27:352–355.
Tessitore N, Mansueto G, Bedogna V et al. A prospective controlled trial on effect of percutaneous transluminal angioplasty on functioning arteriovenous fistulae survival. J Am Soc Nephrol 2003;14:1623–1627.
Tonelli M, Jindal K, Hirsch D, Taylor S, Kane C, Henbrey S. Screening for subclinical stenosis in native vessel arteriovenous fistulae. J Am Soc Nephrol 2001;12:1729–1733.
Trerotola SO, Ponce P, Stavropoulos SW et al. Physical examination versus normalized pressure ratio for predicting outcomes of hemodialysis access interventions. J Vasc Interv Radiol 2003 Nov; 14(11):1387–1394.
Turmel-Rodrigues L, Pengloan J, Rodrigue H et al. Treatment of failed native arteriovenous fistulae for hemodialysis by interventional radiology. Kidney Int 2000;57:1124–1140
9. Время, когда можно использовать (канюлировать) АВ-доступ.
Артериовенозные фистулы
9.1. Мы предполагаем, что артериовенозные фистулы могут быть использованы в качестве АВ-доступа через 4 недели после их формирования у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа, при условии, что при клиническом осмотре они считаются пригодными для канюлирования.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. На практике при клиническом осмотре пригодность для канюлирования определяется наличием пальпируемой вены и ее хорошей вибрацией. Для принятия решения о канюлировании при спорных результатах клинического осмотра может потребоваться ультразвуковое исследование кровотока.
9.2. Не рекомендуем использовать артериовенозную фистулу в качестве АВ-доступа ранее чем через 2 недели после ее формирования, в отношении взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
9.3. Мы предполагаем, что артериовенозные фистулы могут быть использованы в качестве АВ-доступа через 2–4 недели после их формирования у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа, только для того чтобы избежать центрального венозного катетера в качестве сосудистого доступа для гемодиализа.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. Канюлирование под контролем ультразвукового исследования может быть полезным для избежания осложнений и снижения процента неэффективного канюлирования. При раннем канюлировании АВ-доступа использование одноигольного диализа, низкой скорости кровотока во время процедуры диализа и игл меньшего размера (17 размер) может помочь избежать повреждения артериовенозной фистулы.
Allon M, Imrey PB, Cheung AK et al. Relationships between clinical processes and arteriovenous fistula cannulation and maturation: a multicenter prospective cohort study. Am J Kidney Dis 2018;71:677–689.
an Loon MM, Kessels AG, Van der Sande FM, Tordoir JH. Cannulation and vascular access-related complications in hemodialysis: factors determining successful cannulation. Hemodial Int 2009;13:498–504.
Culp K, Flanigan M, Taylor L et al. Vascular access thrombosis in new hemodialysis patients. Am J Kidney Dis 1995;26:341–346.
Ferring M, Henderson J,Wilmink T. Accuracy of early postoperative clinical and ultrasound examination of arteriovenous fistulae to predict dialysis use. J Vasc Access 2014;15:291–297.
Jaberi A, Muradali D, Marticorena RM et al. Arteriovenous fistulas for hemodialysis: application of high-frequency US to assess vein wall morphology for cannulation readiness. Radiology 2011;261:616–624.
Medkouri G, Aghai R, Anabi A et al. Analysis of vascular access in hemodialysis patients: a report from a dialysis unit in Casablanca. Saudi J Kidney Dis Transplant 2006;17:516–520.
Robbin ML, Chamberlain NE, Lockhart ME et al. Hemodialysis arteriovenous fistula maturity: US evaluation. Radiology 2002;225:59–64.
Ravani P, Brunori G, Mandolfo S et al. Cardiovascular comorbidity and late referral impact arteriovenous fistula survival: a prospective multicenter study. J AmSoc Nephrol 2004;15:204–209.
Rayner HC, Pisoni RL, Gillespie BW et al. Creation, cannulation and survival of arteriovenous fistulae: data fromthe dialysis outcomes and practice patterns study. Kidney Int 2003;63:323–330.
Saran R, Dykstra DM, Pisoni RL et al. Timing of first cannulation and vascular access failure in haemodialysis: an analysis of practice patterns at dialysis facilities in the DOPPS. Nephrol Dial Transplant 2004;19:2334–2340.
Wilmink T, Hollingworth L, Stevenson T et al. Is early cannulation of an arteriovenous fistula associated with early failure of the fistula? J Vasc Access 2017;18:92–97.
Wilmink T, Powers S, Hollingworth L et al. Effect of first cannulation time and dialysis machine blood flows on survival of arteriovenous fistulas. Nephrol Dial Transplant 2018;33:841–846.
Wong V, Ward R, Taylor J et al. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur J Vasc Endovasc Surg 1996;12:207–213.
Артериовенозные трансплантаты
9.4. Рекомендуем использовать артериовенозный трансплантат, «предназначенный для ранней канюляции», в качестве АВ-доступа у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа, так рано, как только будет констатировано заживление раны после формирования доступа.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Al Shakarchi J, Inston N. Early cannulation grafts for haemodialysis: an updated systematic review. J Vasc Access 2019;20:123–127.
Chemla ES, Nelson S, Morsy M. Early cannulation grafts in straight axillo-axillary angioaccesses avoid central catheter insertions. Semin Dial 2011;24:456–459.
9.5. Предлагаем использовать артериовенозный трансплантат, «предназначенный для стандартной канюляции», не ранее чем через 2 недели после формирования АВ-доступа у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа, за исключением случаев, когда необходимо избегать центрального венозного катетера в качестве сосудистого доступа для гемодиализа.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Комментарии. Заживление раны означает заживление прилежащих тканей вокруг трансплантата, а не самого участка места разреза. Канюлирование под контролем ультразвукового исследования может быть полезным для избегания осложнений и снижения процента неэффективного канюлирования.
Saran R, Dykstra DM, Pisoni RL et al. Timing of first cannulation and vascular access failure in haemodialysis: an analysis of practice patterns at dialysis facilities in the DOPPS. Nephrol Dial Transplant 2004;19:2334–2340.
Medkouri G, Aghai R, Anabi A et al. Analysis of vascular access in hemodialysis patients: a report from a dialysis unit in Casablanca. Saudi J Kidney Dis Transplant 2006;17:516–520.
Culp K, Flanigan M, Taylor L et al. Vascular access thrombosis in new hemodialysis patients. Am J Kidney Dis 1995;26:341–346.
Sottiurai VS, Stephens A, Champagne L et al. Comparative results of early and delayed cannulation of arteriovenous graft in haemodialysis. Eur J Vasc Endovasc Surg 1997;13:139–141.
Feldman L, Shani M, Mursi J et al. Effect of timing of the first cannulation on survival of arteriovenous hemodialysis grafts. Ther Apher Dial 2013;17:60–64.
Dawidson IJA, Ar’Rajab A, Melone D et al. Early use of the Gore-Tex stretch graft. Blood Purif 1996;14:337–344.
Glickman MH, Burgess J, Cull D et al. Prospective multicenter study with a 1-year analysis of a new vascular graft used for early cannulation in patients undergoing hemodialysis. J Vasc Surg 2015;62:434–441.
Hakaim AG, Scott TE. Durability of early prosthetic dialysis graft cannulation: results of a prospective, nonrandomized clinical trial. J Vasc Surg 1997;25:1002–1005; discussion 1005–1006.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017; 37(Suppl 1):1–191.
10. Техники канюлирования артериовенозных фистул
10.1. Предлагаем не использовать метод одной зоны для канюлирования артериовенозной фистулы у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Комментарии. Антисептические меры и практические аспекты процедуры канюлирования играют важную роль в снижении риска инфекции при «петличной» техники канюлирования.
beas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
Kumwenda M, Mitra S, Reid C. Clinical Practice Guideline – Vascular Access for Haemodialysis, 6th edn. https://renal.org/wp-content/uploads/ 2017/06/vascular-access.pdf. (15 December 2018, date last accessed)
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis 2006;48(Suppl 1):S1–S322.
Nesrallah GE, Mustafa RA, MacRae J et al. Canadian Society of Nephrology guidelines for the management of patients with ESRD treated with intensive hemodialysis. Am J Kidney Dis 2013;62:187–198.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Vale E, Lopez-Vargas P, Polkinghorne K. Nursing Care of Arteriove-nous Fistula/arteriovenous Graft.http://www.cari.org.au/Dialysis/dialysis%20vascular%20access/Nursing_care_of_AVF_AVG. pdf. Accessed 15 December 2018.
10.2. Предлагаем использовать технику «веревочной лестницы» или «петличную» технику для канюлирования артериовенозной фистулы у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа. Основывать свой выбор на локальном опыте и экспертных знаниях медицинского персонала, а также на характеристиках артериовенозной фистулы.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Chow J, Rayment G, San Miguel S et al. A randomised controlled trial of buttonhole cannulation for the prevention of fistula access complications. J RenCare 2011;37:85–93.
Grudzinski A, Mendelssohn D, Pierratos A et al. A systematic review of buttonhole cannulation practices and outcomes. Semin Dial 2013;26:465–475.
MacRae J, Ahmed S, Atkar R et al. A randomized trial comparing buttonhole with rope ladder needling in conventional hemodialysis patients. Clin J Am Soc Nephrol 2012;7:1632–1638.
MacRae J, Ahmed S, Hemmelgarn B. Arteriovenous fistula survival and needling technique: long-term results from a randomized buttonhole trial. Am J Kidney Dis 2014;63:636–642.
Muir CA, Kotwal SS, Hawley CM et al. Buttonhole cannulation and clinical outcomes in a home hemodialysis cohort and systematic review. Clin J Am Soc Nephrol 2014;9:110–119.
Struthers J, Allan A, Peel R et al. Buttonhole needling of ateriovenous fistulae: a randomized controlled trial. ASAIO J 2010;56:319–322.
Toma S, Shinzato T, Fukui H et al. A timesaving method to create a fixed puncture route for the buttonhole technique. Nephrol Dial Transplant 2003;18:2118–212.
Vaux E, King J, Lloyd S et al. Effect of buttonhole cannulation with a polycarbonate PEG on in-center hemodialysis fistula outcomes: a randomized controlled trial. Am J Kidney Dis 2013;62:81–88.
Wong B, Muneer M, Wiebe N et al. Buttonhole versus rope-ladder cannulation of arteriovenous fistulas for hemodialysis: a systematic review. Am J Kidney Dis 2014;64:918–936.
Артериовенозные фистулы
Комментарии. Пациентам с коротким сегментом канюлирования использование «петличной» техники следует предпочесть другим методам.
Ball LK. The buttonhole technique for arteriovenous fistula cannulation. Nephrol Nurs J 2006;33:299–304.
Krönung G. Plastic deformation of Cimino fistula by repeated puncture. Dial Transplant 1984;13:635–638.
Twardowski Z, Kubara H. Different sites versus constant sites of needle insertion into arteriovenous fistulas for treatment by repeated dialysis. Dial Transplant 1979;8:978.
van Loon MM, Kessels AG, Van der Sande FM, Tordoir JH. Cannulation and vascular access-related complications in hemodialysis: factors determining successful cannulation. Hemodial Int 2009;13:498–504.
Wong B, Muneer M, Wiebe N, Storie D, Shurraw S, Pannu N, et al. Buttonhole versus rope-ladder cannulation of arteriovenous fistulas for hemodialysis: a systematic review. Am J Kidney Dis 2014;64:918—936
Артериовенозные трансплантаты
Комментарии. Артериовенозные трансплантаты чаще всего канюлируют при помощи техники «веревочной лестницы».
Brouwer DJ. Cannulation camp: basic needle cannulation training for dialysis staff. Dial Transplant 1995;24:1–7.
McCann M, Einarsdottir H, Van Waeleghem JP, Murphy F, Sedgwick J. Vascular access management II: AVF/AVG cannulation techniques and complications. J Ren Care 2009;35:90–98.
Parisotto MT, Schoder VU, Miriunis C, Grassmann AH, Scatizzi LP, Kaufmann P, et al. Cannulation technique influences arteriovenous fistula and graft survival. Kidney Int 2014;86:
790–797.
11. Типы игл для артериовенозных фистул
11.1. Предлагаем использовать острые иглы или пластиковые канюли для канюлирования артериовенозных фистул у взрослых пациентов при состояниях при ХБП-5, которым показана медицинская помощь методами гемодиализа.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Канюлирование артериовенозных протезов обычно проводят острыми стальными иглами. Программа качественного улучшения техник канюлирования, включая регистрацию и мониторинг типов игл, а также исходов артериовенозного доступа, может помочь при мониторинге качества оказания медицинской помощи, при необходимости способствовать совершенствованию техники канюлирования.
Moore J, Jarvis E. Comparison of large-gauge hollow-bore haemodialysis access needles: a randomised controlled trial. Nephrology 2015; 20:60–89.
Marticorena RM, Dacouris N, Donnelly SM. Randomized pilot study to compare metal needles versus plastic cannulae in the development of complications in hemodialysis access. J Vasc Access 2018;19:272–282.
11.2. Рекомендуем использовать только тупые иглы при применении «петличной» техники канюлирования артериовенозных фистул у взрослых пациентов при состояниях при ХБП–5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Morselli C, Chiari P, Aliberti T et al. Sharp versus blunt dialysis needle use with buttonhole method: open randomised trial. J Renal Care 2015; 41:213–221.
12. Наблюдение за артериовенозным доступом
Артериовенозные фистулы
12.1. Предполагаем, что данных в пользу регулярной оценки АВ-доступа при помощи инструментальных методов исследования в дополнение к клинической оценке функционирующей артериовенозной фистулы с целью выявления и предупреждающей коррекции гемодинамически значимого стеноза артериовенозного доступа у взрослых пациентов при состояниях при ХБП-5 недостаточно и требуется дополнительное изучение.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Aragoncillo I, Abad S, Caldes S et al. Adding access blood flow surveillance reduces thrombosis and improves arteriovenous fistula patency: a randomized controlled trial. J Vasc Access 2017;18:352–358.
Aragoncillo I, Amezquita Y, Caldes S et al. The impact of access blood flow surveillance on reduction of thrombosis in native arteriovenous fistula: a randomized clinical trial. J Vasc Access 2016;17:13–19.
Asif A, Leon C, Orozco-Vargas LC, Krishnamurthy G, Choi KL, Mercado C, et al. Accuracy of physical examination in the detection of arteriovenous fistula stenosis. Clin J Am Soc Nephrol CJASN 2007;2:1191–1194.
Ball LK. Improving arteriovenous fistula cannulation skills. Nephrol Nurs J 2005;32:611–617. quiz 8.
Beathard GA. Physical examination of the dialysis vascular access. Semin Dial 1998;11:231–236.
Campos RP, Chula DC, Perreto S, Riella MC, do Nascimento MM. Accuracy of physical examination and intraaccess pressure in the detection of stenosis in hemodialysis arteriovenous fistula. Semin Dial 2008;21:269–273.
Coentrao L, Faria B, Pestana M. Physical examination of dysfunctional arteriovenous fistulae by non-interventionalists: a skill worth teaching. Nephrol Dial Transplant 2012;27:1993–1996.
Fan PY, Schwab SJ. Vascular access: concepts for the 1990s. J Am Soc Nephrol 1992;3:1–11.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
Jindal K, Chan CT, Deziel C et al. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. J Am Soc Nephrol 2006; 17(3 Suppl 1):S1–S27.
Kumwenda M, Mitra S, Reid C. Clinical Practice Guideline – Vascular Access for Haemodialysis, 6th edn. https://renal.org/wp-content/uploads/ 2017/06/vascular-access.pdf. (15 December 2018, date last accessed).
Leon C, Asif A. Physical examination of arteriovenous fistulae by a renal fellow: does it compare favorably to an experienced interventionalist? Semin Dial 2008;21:557–560.
Mestres G, Fontsere N, Garcia-Madrid C, Campelos P, Maduell F, Riambau V. Intra-operative factors predicting 1-month arteriovenous fistula thrombosis. J Vasc Access 2012;13:193e7.
National Institute for Health and Care Excellence. Renal Replacement Therapy Services for Adults. NICE Guideline QS72. https://www.nice.org. uk/guidance/qs72. (15 December 2018, date last accessed).
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis 2006;48(Suppl 1): S1–S322.
Ravani P, Quinn RR, Oliver MJ et al. Pre-emptive correction for haemodialysis arteriovenous access stenosis. Cochrane Database Syst Rev 2016;1:CD010709.
Salman L, Beathard G. Interventional nephrology: Physical examination as a tool for surveillance for the hemodialysis arteriovenous access. Clin J Am Soc Nephrol CJASN 2013;8:1220–1227.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Schuman E, Ronfeld A, Barclay C, Heinl P. Comparison of clinical assessment with ultrasound flow for hemodialysis access surveillance. Arch Surg 2007;142:1129–1133.
Артериовенозные трансплантаты
12.2. Не предполагаем, что следует проводить техническое наблюдение при помощи инструментальных методов исследования в дополнение к клинической оценке функционирующего артериовенозного трансплантата с целью выявления и предупреждающей коррекции гемодинамически значимого стеноза артериовенозного доступа у взрослых при состояниях при ХБП-5, кроме случаев, когда это осуществляется в контексте клинического исследования.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Fan PY, Schwab SJ. Vascular access: concepts for the 1990s. J Am Soc Nephrol 1992;3:1–11.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017; 37(Suppl 1):1–191
Jindal K, Chan CT, Deziel C et al. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. J Am Soc Nephrol 2006; 17(3 Suppl 1):S1–S27.
Kumwenda M, Mitra S, Reid C. Clinical Practice Guideline – Vascular Access for Haemodialysis, 6th edn. https://renal.org/wp-content/uploads/ 2017/06/vascular-access.pdf. (15 December 2018, date last accessed)
Leon C, Orozco-Vargas LC, Krishnamurthy G, Choi KL, Mercado C, Merrill D, et al. Accuracy of physical examination in the detection of arteriovenous graft stenosis. Semin Dial 2008;21:85–88.
May RE, Himmelfarb J, Yenicesu M, Knights S, Ikizler TA, Schulman G, et al. Predictive measures of vascular access thrombosis: a prospective study. Kidney Int 1997;52:1656–1662.
McCarley P, Wingard RL, Shyr Y, Pettus W, Hakim RM, Ikizler TA. Vascular access blood flow monitoring reduces access morbidity and costs. Kidney Int 2001;60:1164–1172.
National Institute for Health and Care Excellence. Renal Replacement Therapy Services for Adults. NICE Guideline QS72. https://www.nice.org. uk/guidance/qs72. (15 December 2018, date last accessed).
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis 2006; 48(Suppl 1): S1–S322.
Ravani P, Quinn RR, Oliver MJ et al. Pre-emptive correction for haemodialysis arteriovenous access stenosis. Cochrane Database Syst Rev 2016;1:CD010709.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Smits JH, van der Linden J, Hagen EC, ModderkolkCammeraat EC, Feith GW, Koomans HA, et al. Graft surveillance: venous pressure, access flow, or the combination? Kidney Int 2001;59:1551–1558.
13. Хирургические и рентгенэндоваскулярные вмешательства при несозревании артериовенозных фистул
13.1. Предполагаем, что существует недостаточно данных в пользу открытых хирургических вмешательств перед рентгенэндоваскулярными вмешательствами в качестве предпочтительного метода терапии при несозревании артериовенозных фистул у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. При выявлении задержки или отсутствии созревания АВ-фистулы через 4–6 недель от времени формирования АВ-фистулы необходимо провести клиническое обследование и получить подтверждение предполагаемого отсутствия созревания при помощи инструментальных методов исследования с последующим плановым лечением. Решения о методах лечения при несозревании артериовенозных фистул лучше всего принимать с учетом местных ресурсов, клинического опыта врача-специалиста и процента эффективности вмешательств. В медицинских организациях целесообразно формировать специализированную мультидисциплинарную команду для создания сосудистого доступа, состоящую из специалистов, имеющих клинический опыт и практические навыки в различных методах коррекции несозревания артериовенозных фистул.
DerDerian T, Hingorani A, Boniviscage P et al. Acute complications after balloon-assisted maturation. Ann Vasc Surg 2014;28:1275–1279.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
Ives CL, Akoh JA, George J, Vaughan-Huxley E, Lawson H. Preoperative vessel mapping and early post-operative surveillance duplex scanning of arteriovenous fistulae. J Vasc Access 2009;10:37–42.
Lee T, Tindni A, Roy-Chaudhury P. Improved cumulative survival in fistulas requiring surgical interventions to promote fistula maturation compared with endovascular interventions. Semin Dial 2013;26:85–89.
Long B, Brichart N, Lermusiaux P et al. Management of perianastomotic stenosis of direct wrist autogenous radial-cephalic arteriovenous accesses for dialysis. J Vasc Surg 2011;53:108–114.
Saran R, Pisoni RL, Young EW. Timing of first cannulation of arteriovenous fistula: are we waiting too long? Nephrol Dial Transplant 2005;20:688–690.
Tordoir JHM, Zonnebeld N, van Loon MM et al. Surgical and endovascular intervention for dialysis access maturation failure during and after arteriovenous fistula surgery: review of the evidence. Eur J Vasc Endovasc Surg 2018;55:240–248.
14. Медицинская помощь для поддержания долгосрочной проходимости артериовенозного доступа
Артериовенозные фистулы
14.1. Предполагаем, что любое решение о назначении рыбьего жира взрослым пациентам при состояниях при ХБП-5 в течение первого года после формирования артериовенозной фистулы должно соблюдать баланс между улучшением проходимости через 1 год после оперативного вмешательства с непредвиденным риском кровотечения или других побочных эффектов.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Tanner NC, Da Silva A. Medical adjuvant treatment to increase patency of arteriovenous fistulae and grafts. Cochrane Database Syst Rev 2015;7:CD002786.
Viecelli AK, Irish AB, Polkinghorne KR et al. Omega-3 polyunsaturated fatty acid supplementation to prevent arteriovenous fistula and graft failure: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis 2018;72:50–61.
14.2. Предполагаем, что длинноволновая инфракрасная терапия может быть рассмотрена в целях улучшения долгосрочной проходимости артериовенозной фистулы у взрослых при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Bashar K, Healy D, Browne LD et al. Role of far infra-red therapy in dialysis arterio-venous fistula maturation and survival: systematic review and meta-analysis. PLoS One 2014;9:e104931.
Wan Q, Yang S, Li L et al. Effects of far infrared therapy on arteriovenous fistulas in hemodialysis patients: a meta-analysis. Renal Failure 2017;39:613–622.
14.3. Недостаточно данных рандомизированных контролируемых исследований для рекомендации аспирина, клопидогрела, тиклопидина, варфарина, сульфинпиразона, вонапанитазы, берапроста натрия, холекальциферола, статинов, дипиридамола или дипиридамола в сочетании с аспирином для поддержания долгосрочной проходимости артериовенозной фистулы у взрослых при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Abacilar AF, Atalay H, Dogan OF. Oral prostacycline analog and clopidogrel combination provides early maturation and long-term survival after arteriovenous fistula creation: a randomized controlled study. Indian J Nephrol 2015;25:136–142. Abacilar AF, Atalay H, Dogan OF. Oral prostacycline analog and clopidogrel combination provides early maturation and long-term survival after arteriovenous fistula creation: a randomized controlled study. Indian J Nephrol 2015;25:136–142.
Bleyer A, Kidd K, Wilson S et al. The effect of topically applied vonapanitase on fistula outcomes: results of the patency-1 trial. Am J Kidney Dis 2017;69:A2.
Harter HR, Burch JW, Majerus PW et al. Prevention of thrombosis in patients on hemodialysis by low-dose aspirin. N Engl J Med 1979;301:577–557.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
Kim M, Kim JU, Kim SM et al. Effectiveness of beraprost sodium in maintaining vascular access patency in patients on hemodialysis. Int Urol Nephrol 2017;49:1287–1295.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55:757–818.
Tanner NC, Da Silva A. Medical adjuvant treatment to increase patency of arteriovenous fistulae and grafts. Cochrane Database Syst Rev 2015;7:CD002786.
Артериовенозные протезы
14.4. Не рекомендуем назначения варфарина в комбинации с антитромбоцитарными препаратами, а также клопидогрела в сочетании с аспирином в высоких дозах для снижения риска тромбоза артериовенозного трансплантата у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств I, уровень убедительности рекомендаций C
Crowther MA, Clase CM, Margetts PJ et al. Low-intensity warfarin is ineffective for the prevention of PTFE graft failure in patients on hemodialysis: a randomized controlled trial. J Am Soc Nephrol 2002;13:2331–2337.
Kaufman JS, Connor TZ, Zhang JH et al. Randomized controlled trial of clopidogrel plus aspirin to prevent hemodialysis access graft thrombosis. J AmSocNephrol 2003;14:2313–2321.
Palmer SC, Di Micco L, Razavian M et al. Antiplatelet agents for chronic kidney disease. Cochrane Database Syst Rev 2013;4:CD008834.
Tanner NC, Da Silva A. Medical adjuvant treatment to increase patency of arteriovenous fistulae and grafts. Cochrane Database Syst Rev 2015;7:CD002786.
14.5. Предполагаем, что любое решение о назначении рыбьего жира взрослым пациентам при состояниях при ХБП-5 в течение первого года после формирования артериовенозной трансплантата должно соблюдать баланс между улучшением проходимости через 1 год после оперативного вмешательства с непредвиденным риском кровотечения.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Viecelli AK, Irish AB, Polkinghorne KR et al. Omega-3 polyunsaturated fatty acid supplementation to prevent arteriovenous fistula and graft failure: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis 2018;72:50–61.
14.6. Недостаточно данных рандомизированных контролируемых исследований для рекомендации аспирина, клопидогрела, тиклопидина, варфарина, берапроста натрия, статинов, дипиридамола или дипиридамола в сочетании с аспирином для поддержания долгосрочной проходимости артериовенозного трансплантата у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Harter HR, Burch JW, Majerus PW et al. Prevention of thrombosis in patients on hemodialysis by low-dose aspirin. N Engl J Med 1979;301:577–579.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
KimM, Kim JU, Kim SM et al. Effectiveness of beraprost sodium in maintaining vascular access patency in patients on hemodialysis. Int Urol Nephrol 2017;49:1287–1295.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Sreedhara R, Himmelfarb J, Lazarus J et al. Anti-platelet therapy in graft thrombosis: results of a prospective, randomized, double-blind study.Kidney Int 1994;45:1477–1483.
15. Время для вмешательства при тромбозе артериовенозной фистулы
15.1. Предлагаем попытаться в оптимальные сроки и как можно быстрее удалить тромб из АВ-фистулы до проведения очередной процедуры гемодиализа у взрослых при состояниях при ХБП-5.
Уровень достоверности доказательств I, уровень убедительности рекомендаций C
Комментарии. Для спасения сосудистого доступа при раннем тромбозе тромбэктомия и ревизия (при необходимости) должны быть выполнены так скоро, как это возможно. При раннем тромбозе не следует использовать тромболизис в течение 7 дней с момента создания сосудистого доступа.
Beathard GA. Successful treatment of the chronically thrombosed dialysis access graft: resuscitation of dead grafts. Semin Dial 2006;19:417–420.
Diskin CJ, Stokes TJ, Panus LWet al. The importance of timing of surgery for hemodialysis vascular access thrombectomy. Nephron 1997;75:233–237.
Green LD, Lee DS, Kucey DS. A metaanalysis comparing surgical thrombectomy, mechanical thrombectomy, and pharmacomechanical thrombolysis for thrombosed dialysis grafts. J Vasc Surg 2002;36:939–945.
Ibeas J, Roca-Tey R, Vallespin J et al. Spanish clinical guidelines on vascular access for haemodialysis. Guia Clinica Espanola Del Acceso Vascular Para Hemodialisis 2017;37(Suppl 1):1–191.
Kuhan G, Antoniou GA, Nikam M, Mitra S, Farquharson F, Brittenden J, et al. A meta-analysis of randomized trials comparing surgery versus endovascular therapy for thrombosed arteriovenous fistulas and grafts in hemodialysis. Cardiovasc Intervent Radiol 2013;36:699–705.
Kumwenda M, Mitra S, Reid C. Clinical Practice Guideline – Vascular Access for Haemodialysis, 6th edn. https://renal.org/wp-content/uploads/ 2017/06/vascular-access.pdf. (15 December 2018, date last accessed).
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis 2006; 48(Suppl 1): S1–S322
Sadaghianloo N, Jean-Baptiste E, Gaid H et al. Early surgical thrombectomy improves salvage of thrombosed vascular accesses. J Vasc Surg 2014;59:1377–1384.e2.
Schmidli J,Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Shemesh D, Goldin I, Berelowitz D, Zaghal I, Olsha O. Thrombolysis for early failure of prosthetic arteriovenous access. J Vasc Surg 2008;47:585–590.
Tordoir JH, Bode AS, Peppelenbosch N, van der Sande FM, de Haan MW. Surgical or endovascular repair of thrombosed dialysis vascular access: is there any evidence? J Vasc Surg 2009;50:953–956.
15.2. Предлагаем попытаться удалить тромб из артериовенозной фистулы у взрослых пациентов при состояниях при ХБП-5, даже если имела место задержка на несколько дней или недель.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
El-Damanawi R, Kershaw S, Campbell G et al. Successful restoration of arteriovenous dialysis access patency after late intervention. Clin Kidney J 2015;8:82–86.
Graor RA, Risius B, Denny KM et al. Local thrombolysis in the treatment of thrombosed arteries, bypass grafts, and arteriovenous fistulas. J Vasc Surg 1985; 2: 406–414.
16. Хирургические и рентгенэндоваскулярные вмешательства при тромбозе артериовенозного доступа
16.1. Предлагаем основывать выбор между хирургическим и рентгенэндоваскулярным вмешательством при тромбозе артериовенозного доступа на состоянии пациента и функционировании сосудистого доступа, а также на наличии локального опыта и экспертных знаний медицинского персонал ввиду отсутствия преимущества одного подхода над другим.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Лечение тромбоза сосудистого доступа должно включать периоперационную диагностику и лечение любого ассоциированного стеноза.
Barth KH, Gosnell MR, Palestrant AM et al. Hydrodynamic thrombectomy system versus pulse-spray thrombolysis for thrombosed hemodialysis grafts: a multicenter prospective randomized comparison. Radiology 2000;217:678–684.
Crikis S, Lee D, Brooks M, Power DA, Ierino FL, Levidiotis V. Predictors of early dialysis vascular-access failure after thrombolysis. Am J Nephrol 2008;28:181e9.
Kuhan G, Antoniou GA, Nikam M, Mitra S, Farquharson F, Brittenden J, et al. A meta-analysis of randomized trials comparing surgery versus endovascular therapy for thrombosed arteriovenous fistulas and grafts in hemodialysis. Cardiovasc Intervent Radiol 2013;36:699–705.
Smits HF, Smits JH, Wust AF, Buskens E, Blankestijn PJ. Percutaneous thrombolysis of thrombosed haemodialysis access grafts: comparison of three mechanical devices. Nephrol Dial Transplant 2002;17:467–473.
Tordoir JH, Bode AS, Peppelenbosch N, van der Sande FM, de Haan MW. Surgical or endovascular repair of thrombosed dialysis vascular access: is there any evidence? J Vasc Surg 2009;50:953–956.
Turmel-Rodrigues L, Pengloan J, Rodrigue H, Brillet G, Lataste A, Pierre D, et al. Treatment of failed native arteriovenous fistulae for hemodialysis by interventional radiology. Kidney Int 2000;57:1124–1140.
Uflacker R, Rajagopalan P, Selby J et al. Thrombosed dialysis access grafts: randomized comparison of the Amplatz thrombectomy device and surgical thromboembolectomy. Eur Radiol 2004;14:2009–2014.
Vogel PM, Bansal V, Marshall MW. Thrombosed hemodialysis grafts: lyse and wait with tissue plasminogen activator or urokinase compared to mechanical thrombolysis with the Arrow-Trerotola percutaneous thrombolytic device. J Vasc Interv Radiol 2001;12:1157–1165.
17. Диагностика и лечение стеноза АВ-доступа
17.1. Предлагаем выполнить визуализацию как можно скорее, если подозревается гемодинамически значимый стеноз АВ-доступа при клиническом осмотре и/или при измерении потока крови.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Комментарии. При снижении эффективности гемодиализа следует рассмотреть вопрос об исследовании и коррекции на предмет стеноза сосудистого доступа.
Hakim RM, Breyer J, Ismail N, Schulman G. Effects of dose of dialysis on morbidity and mortality. Am J Kidney Dis 1994;23: 661–669.
Sehgal AR, Dor A, Tsai AC. Morbidity and cost implications of inadequate hemodialysis. Am J Kidney Dis 2001;37:1223–1231.
Tonelli M, Jhangri GS, Hirsch DJ, Marryatt J, Mossop P, Wile C, et al. Best threshold for diagnosis of stenosis or thrombosis within six months of access flow measurement in arteriovenous fistulae. J Am Soc Nephrol 2003;14:3264–3269.
Trerotola SO, Stavropoulos SW, Shlansky-Goldberg R, Tuite CM, Kobrin S, Rudnick MR. Hemodialysis-related venous stenosis: treatment with ultrahigh-pressure angioplasty balloons. Radiology 2004;231:259–262.
Windus DW, Audrain J, Vanderson R, Jendrisak MD, Picus D, Delmez JA. Optimization of high-efficiency hemodialysis by detection and correction of fistula dysfunction. Kidney Int 1990;38:337–341.
Комментарии. Ультразвуковое дуплексное сканирование рекомендуется в качестве первой линии визуализации при подозрении на дисфункцию сосудистого доступа. При неубедительных данных УЗИ или ангиографии относительно степени центрального венозного стеноза компьютерная томографическая ангиография должна быть выполнена. При дисфункции АВ-доступа числовая субтракционная ангиография должна выполняться только в том случае, если в последующем ожидается вмешательство. Магнитно-резонансная ангиография с контрастом не рекомендуется пациентам ХБП из-за потенциального риска.
Dimopoulou A, Raland H, Wikstrom B, Magnusson A. MDCT angiography with 3D image reconstructions in the evaluation of failing arteriovenous fistulas and grafts in hemodialysis patients. Acta Radiol 2011;52:935e42.
Doelman C, Duijm LEM, Liem YS et al. Stenosis detection in failing hemodialysis access fistulas and grafts: Comparison of color Doppler ultrasonography, contrast-enhanced magnetic resonance angiography, and digital subtraction angiography. J Vasc Surg 2005;42:739–746.
Grobner T. Gadoliniumea specific trigger for the development of nephrogenic fibrosing dermopathy and nephrogenic systemic fibrosis? Nephrol Dial Transplant 2006;21:1104–1108.
Gadallah MF, Paulson WO, Vickers B, Work J. Accuracy of Doppler ultrasound in diagnosing anatomic stenosis of hemodialysis arteriovenous access as compared with fistulography. Am J Kidney Dis 1998;32:273–27.7.
Karadeli E, Tarhan NC, Ulu EM, Tutar NU, Basaran O, Coskun M, et al. Evaluation of failing hemodialysis fistulas with multidetector CT angiography: comparison of different 3D planes. Eur J Radiol 2009;69:184–192.
MacDonald MJ, Martin LG, Hughes JD, Kikeri D, Scout DC, Harker LA. Distribution and severity of stenoses in functioning arteriovenous grafts: a duplex and angiographic study. J Vasc Technol 1996;20:131–136.
Rooijens PP, Serafino GP, Vroegindeweij D, Dammers R, Yo TI, De Smet AA, et al. Multi-slice computed tomographic angiography for stenosis detection in forearm hemodialysis arteriovenous fistulas. J Vasc Access 2008;9:278e84.
Schwarz C, Mitterbauer C, Boczula M, Maca T, Funovics M, Heinze G, et al. Flow monitoring: performance characteristics of ultrasound dilution versus color Doppler ultrasound compared with fistulography. Am J Kidney Dis 2003;42:539–545.
Shackleton CA, Taylor OC, Buckley AR, Rowley VA, Cooperberg PL, Fry PD. Predicting failure in polytetrafluoroethylene vascular access grafts for hemodialysis: a pilot study. Can J Surg 1987;30:442–444.
Tordoir JH, de Bruin HG, Hoeneveld H, Eikelboom BC, Kitslaar PJ. Duplex ultrasound scanning in the assessment of arteriovenous fistulas created for hemodialysis access: comparison with digital subtraction angiography. J Vasc Surg 1989;10:122–128.
Tordoir JH, Hoeneveld H, Eikelboom BC, Kitslaar PJ. The correlation between clinical and duplex ultrasound parameters and the development of complications in arteriovenous fistulae for haemodialysis. Eur J Vasc Surg 1990; 4:179–184.
Turmel-Rodrigues L, Pengloan J, Bourquelot P. Interventional radiology in hemodialysis fistulae and grafts: a multidisciplinary approach. Cardiovasc Intervent Radiol 2002; 25:3–16.
Wasinrat J, Siriapisith T, Thamtorawat S, Tongdee T. 64-slice MDCT angiography of upper extremity in assessment of native hemodialysis access. Vasc Endovasc Surg 2011;45:69e77.
17.2. Предлагаем при стенозе АВ-доступа выполнять превентивное вмешательство хирургическим и рентгенэндоваскулярным методами, выбор которых основывается на наличии локального опыта и экспертных знаниях медицинского персонала.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. Каждый центр должен оценивать свои результаты и выбирать вид оперативного вмешательства для достижения наилучших результатов. Изменение протоколов возможно в зависимости от изменения результатов. Как правило, визуализация должна быть выполнена непосредственно перед вмешательством.
Haage P, Vorwerk D, Piroth W, Schu¨rmann K, Gu¨nther RW. Treatment of hemodialysis-related central venous stenosis or occlusion: results of primary Wallstent placement and follow-up in 50 patients. Radiology 1999;212:175–180.
Le Blanche AF, Tassart M, Deux JF, Rossert J, Bigot JM, Boudghene F. Gadolinium-enhanced digital subtraction angiography of hemodialysis fistulas: a diagnostic and therapeutic approach. AJR Am J Roentgenol 2002;179:1023–1028.
Duijm LE, Liem YS, van der Rijt RH et al. Inflow stenoses in dysfunctional hemodialysis access fistulae and grafts. Am J Kidney Dis 2006;48:98–105.
Комментарии. Рентгенэндоваскулярные методы лечения возможны при их наличии как первый вариант при нарушении оттока при венозном стенозе.
Besarab A. Preventing vascular access dysfunction: which policy to follow. Blood Purif 2002;20:26–35.
Casey ET, Murad MH, Rizvi AZ, Sidawy AN, McGrath MM, Elamin MB, et al. Surveillance of arteriovenous hemodialysis access: a systematic review and meta-analysis. J Vasc Surg 2008;48:48S–54S.
Clark TW, Hirsch DA, Jindal KJ, Veugelers PJ, LeBlanc J. Outcome and prognostic factors of restenosis after percutaneous treatment of native hemodialysis fistulas. J Vasc Interv Radiol 2002;13:51–59.
Haage P, Vorwerk D, Wildberger JE, Piroth W, Schu¨rmann K, Gu¨nther RW. Percutaneous treatment of thrombosed primary arteriovenous hemodialysis access fistulae. Kidney Int 2000; 57:1169–1175.
Bakken AM, Protack CD, Saad WE, Lee DE, Waldman DL, Davies MG. Long-term outcomes of primary angioplasty and primary stenting of central venous stenosis in hemodialysis patients. J Vasc Surg 2007;45:776–783 (17398386).
Hoffer EK, Sultan S, Herskowitz MM, Daniels ID, Sclafani SJ. Prospective randomized trial of a metallic intravascular stent in hemodialysis graft maintenance. J Vasc Intervent Radiol JVIR 1997;8:965–973.
Lay JP, Ashleigh RJ, Tranconi L, Ackrill P, Al-Khaffaf H. Result of angioplasty of brescia-cimino haemodialysis fistulae: medium-term follow-up. Clinical Radiology 1998;53:608–611.
Romero A, Polo JR, Garcia ME, Garcia Sabrido JL, Quintans A, Ferreira JP. Salvage of angioaccess after late thrombosis of radiocephalic fistulas for hemodialysis. Int Surg 1986;71:122–124.
Sugimoto K, Higashino T, Kuwata Y, Imanaka K, Hirota S, Sugimura K. Percutaneous transluminal angioplasty of malfunctioning Brescia-Cimino arteriovenous fistula: analysis of factors adversely affecting long-term patency. Eur Radiol 2003;13:1615–1619.
Tessitore N, Mansueto G, Bedogna V, Lipari G, Poli A, Gammaro L, et al. A prospective controlled trial on effect of percutaneous transluminal angioplasty on functioning arteriovenous fistulae survival. J Am Soc Nephrol 2003;14: 1623–1627.
Tonelli M, James M, Wiebe N, Jindal K, Hemmelgarn B. Ultrasound monitoring to detect access stenosis in hemodialysis patients: a systematic review. Am J Kidney Dis 2008;51:630–640.
Tonelli M, Jhangri GS, Hirsch DJ, Marryatt J, Mossop P, Wile C, et al. Best threshold for diagnosis of stenosis or thrombosis within six months of access flow measurement in arteriovenous fistulae. J Am Soc Nephrol 2003;14:3264–3269.
Trerotola SO, Stavropoulos SW, Shlansky-Goldberg R, Tuite CM, Kobrin S, Rudnick MR. Hemodialysis-related venous stenosis: treatment with ultrahigh-pressure angioplasty balloons. Radiology 2004;231:259–262.
Turmel-Rodrigues L, Pengloan J, Baudin S et al. Treatment of stenosis and thrombosis in haemodialysis fistulas and grafts by interventional radiology. Nephrol Dial Transplant 2000;15:2029–2036.
Turmel-Rodrigues L, Pengloan J, Blanchier D et al. Insufficient dialysis shunts: improved long-term patency rates with close hemodynamic monitoring, repeated percutaneous balloon angioplasty, and stent placement. Radiology 1993;187:273–278.
Turmel-Rodrigues L, Raynaud A, Bourquelot P. Percutaneous treatment of arteriovenous access dysfunction. In: Conlon PJ, Schwab SJ, Nicholson ML, eds. Hemodialysis Vascular Access: Practice and Problems. Oxford University Press, Oxford; New York 2000;183–202.
Vorwerk D, Adam G, Mu¨ller-Leisse C, Gu¨nther RW. Hemodialysis fistulas and grafts: use of cutting balloons to dilate venous stenoses. Radiology 1996;201:864–867.
Vorwerk D, Bu¨cker A, Alzen G, Schu¨rmann K, Ritzerfeld M, Gu¨nther RW. Chronic venous occlusions in haemodialysis shunts: efficacy of percutaneous treatment. Nephrol Dial Transpl 1995;10:1869–1873.
Комментарии. Рентгенэндоваскулярные методы лечения (баллонная ангиопластика) возможны при их наличии в качестве основного средства лечения при артериальном стенозе притока любого типа сосудистого доступа.
Asif A, Gadalean FN, Merrill D, Cherla G, Cipleu CD, Epstein DL, et al. Inflow stenosis in arteriovenous fistulas and grafts: a multicenter, prospective study. Kidney Int 2005;67:1986–1992.
Duijm LE, Liem YS, van der Rijt RH, Nobrega FJ, van den Bosch HC, Douwes-Draaijer P, et al. Inflow stenoses in dysfunctional hemodialysis access fistulae and grafts. Am J Kidney Dis 2006;48:98–105.
Комментарии. При стенозе анастомоза на предплечье необходимо выполнить хирургическое вмешательство для проксимального перемещения анастомоза сосудистого доступа.
Jimenez-Almonacid P, Gruss-Vergara E, Jimenez-Toscano M, Lasala M, Rueda JA, Portoles J, et al. Surgical treatment of juxtaanastomotic stenosis in radiocephalic fistula. A new proximal radiocephalic anastomosis. Nefrologia 2012;32:517–522.
18. Диагностика и лечение центральной венозной окклюзии
18.1. Предлагаем выполнять ангиографию доступа из вены, по которой осуществляется отток, при наличии симптомов и подозрении на центральную венозную окклюзию.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. При наличии стойкого отека руки после создания сосудистого доступа для оценки ипсилатерального центрального венозного оттока рекомендуется фистулография или компьютерная томография с ангиографией.
Beathard GA. Mechanical versus pharmacomechanical thrombolysis for the treatment of thrombosed dialysis access grafts. Kidney Int 1994;45:1401–1406.
Bhatia DS, Money SR, Ochsner JL et al. Comparison of surgical bypass and percutaneous balloon dilatation with primary stent placement in the treatment of central venous obstruction in the dialysis patient: one-year follow-up. Ann Vasc Surg 1996;10:452–455.
Dammers R, de Haan MW, Planken NR, van der Sande FM, Tordoir JH. Central vein obstruction in hemodialysis patients: results of radiological and surgical intervention. Eur J Vasc Endovasc 2003;26:317–321.
Davis JE, Sugioka K. Selecting the patient for major ambulatory surgery. Surgical and anesthesiology evaluations. Surg Clin North Am 1987;67:721–732.
Haage P, Vorwerk D, Piroth W, Schu¨rmann K, Gu¨nther RW. Treatment of hemodialysis-related central venous stenosis or occlusion: results of primary Wallstent placement and follow-up in 50 patients. Radiology 1999; 212 175–180.
Kalman PG, Lindsay TF, Clarke K, Sniderman KW, Vanderburgh L. Management of upper extremity central venous obstruction using interventional radiology. Ann Vasc Surg 1998;12:202–206.
Kovalik EC, Newman GE, Suhocki P, Knelson M, Schwab SJ. Correction of central venous stenoses: use of angioplasty and vascular Wallstents. Kidney Int 1994;45:1177–1181.
Labropoulos N, Borge M, Pierce K, Pappas PJ. Criteria for defining significant central vein stenosis with duplex ultrasound. J Vasc Surg 2007;46:101–107 (17540535).
Landwehr P, Tschammler A, Schaefer RM, Lackner K. The value of color-coded duplex sonography of a dialysis shunt. Rofo Fortschr Geb Ro¨ntgenstr Neuen Bildgeb Verfahr 1990;153:185–191.
Mickley V. Central vein obstruction in vascular access. Eur J Vasc Endovasc Surg 2006;32:439–444 (16765068).
Mickley V. Stent or bypass? Treatment results in benign central venous obstruction. Zentralbl Chir 2001;126:445–449.
Money S, Bhatia D, Daharamsay S, Mulingtapan R, Shaw D, Ramee S. Comparison of surgical by-pass, percutaneous balloon dilatation (PTA) and PTA with stent placement in the treatment of venous occlusion in the dialysis patient. One year follow up. Int Angiol 1995;14:176.
Oderich GS, Treiman GS, Schneider P, Bhirangi K. Stent placement for treatment of central and peripheral venous obstruction: a long-term multi-institutional experience. J Vasc Surg 2000;32:760–769.
Quinn SF, Schuman ES, Demlow TA et al. Percutaneous transluminal angioplasty versus endovascular stent placement in the treatment of venous stenoses in patients undergoing hemodialysis: intermediate results. J Vasc Interv Radiol 1995;6:851–855.
Sprouse II, LR, Lesar CJ, Meier III, GH et al. Percutaneous treatment of symptomatic central venous stenosis. J Vasc Surg 2004;39:578–582.
18.2. Предлагаем выполнять рентгенэндоваскулярные методы лечения при центральной венозной окклюзии.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. Рекомендуется баллонная ангиопластика как первичное симптоматическое лечение, повторное вмешательство по показаниям. Если после баллонной ангиопластики наблюдается значительное уменьшение просвета центральной вены или повторяется стеноз в течение 3 месяцев, необходимо повторение баллонной ангиопластики или стентирование.
Anaya-Ayala JE, Smolock CJ, Colvard BD, Naoum JJ, Bismuth J, Lumsden AB, et al. Efficacy of covered stent placement for central venous occlusive disease in hemodialysis patients. J Vasc Surg 2011;54:754–759.
Bakken AM, Protack CD, Saad WE, Lee DE, Waldman DL, Davies MG. Long-term outcomes of primary angioplasty and primary stenting of central venous stenosis in hemodialysis patients. J Vasc Surg 2007;45:776–783 (17398386).
Dracon M, Watine O, Pruvot F, Noel C, Lelievre G. Axillo-axillary access in hemodialysis. Nephrologie 1994;15:175–176.
El-Sabrout RA, Duncan JM. Right atrial bypass grafting for central venous obstruction associated with dialysis access: another treatment option. J Vasc Surg 1999;29:472–478.
Kavallieratos N, Kokkinos A, Kalocheretis P. Axillary to saphenous vein bypass for treatment of central venous obstruction in patients receiving dialysis. J Vasc Surg 2004;40:640–643.
Kim YC, Won JY, Choi SY, Ko H-K, Lee K-H, Lee DY, et al. Percutaneous treatment of central venous stenosis in hemodialysis patients: long-term outcomes. Cardiovasc Intervent Radiol 2009;32:271–278 (19194745).
Kundu S, Modabber M, You JM, Tam P, Nagai G, Ting R. Use of PTFE stent grafts for hemodialysis-related central venous occlusions: intermediate-term results. Cardiovasc Intervent Radiol 2011;34:949–957 (21069331).
Kundu S. Review of central venous disease in hemodialysis patients. J Vasc Intervent Radiol JVIR 2010;21:963–968.
Maya ID, Saddekni S, Allon M. Treatment of refractory central vein stenosis in hemodialysis patients with stents. Semin Dial 2007;20:78–82.
Ono K, Muto Y, Yano K, Yukizane T. Anterior chest wall axillary artery to contralateral axillary vein graft for vascular access in hemodialysis. Artif Organs 1995;19:1233–1236.
Ozyer U, Harman A, Yildirim E, Aytekin C, Karakayali F, Boyvat F. Long-term results of angioplasty and stent placement for treatment of central venous obstruction in 126 hemodialysis patients: a 10-year single-center experience. AJR Am J Roentgenol 2009;193:1672–1679 (19933663).
Quaretti P, Galli F, Moramarco LP, Corti R, Leati G, Fiorina I, et al. Stent grafts provided superior primary patency for central venous stenosis treatment in comparison with angioplasty and bare metal stent: a retrospective single center study on 70 hemodialysis patients. Vasc Endovasc Surg 2016;50:221–230.
Ronald J, Davis B, Guevara CJ, Pabon-Ramos WM, Smith TP, Kim CY. Treatment of central venous in-stent restenosis with repeat stent deployment in hemodialysis patients. J Vasc Access 2017;18:214–219.
Sottiurai VS, Stephens A, Champagne L, Reisen E. Preservation of hemodialysis access with central obstruction. Int J Angiol 1996;5:171–174.
19. Диагностика и лечение ишемии конечности, вызванной АВ-доступом
19.1. Предлагаем диагностировать ишемию, вызванную АВ-доступом, при клиническом мониторинге, и причина должна быть идентифицирована неинвазивными методами визуализации и ангиографией.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. Послеоперационный клинический мониторинг признаков ишемической невропатии рекомендуется пациентам с сахарным диабетом или наличием в анамнезе невропатии, у которых сформирован доступ на плече.
Davidson D, Louridas G, Guzman R et al. Steal syndrome complicating upper extremity hemoaccess procedures: incidence and risk factors. Can J Surg 2003;46:408–412.
Duncan H, Ferguson L, Faris I. Incidence of the radial steal syndrome in patients with Brescia fistula for hemodialysis: its clinical significance. J Vasc Surg 1986;4:144–147.
Henriksson AE, Bergqvist D. Steal syndrome of the hemodialysis vascular access: Diagnosis and treatment. J Vasc Access 2004;5:62–68.
Khan FA, Vesely TM. Arterial problems associated with dysfunctional hemodialysis grafts: evaluation of patients at high risk for arterial disease. J Vasc Interv Radiol 2002;13:1109–1114.
Lazarides MK, Staramos DN, Kopadis G, Maltezos C, Tzilalis VD, Georgiadis GS. Onset of arterial ‘steal’ following proximal angioaccess: immediate and delayed types. Nephrol Dial Transplant 2003;18:2387–2390.
Lazarides MK, Staramos DN, Panagopoulos GN et al. Indications for surgical treatment of angioaccess-induced arterial ‘steal’. J Am Coll Surg 1998;187:422–426.
Levine MP. The hemodialysis patient and hand amputation. Am J Nephrol 2001;21:498–501.
Morsy AH, Kulbaski M, Chen C, Isiklar H, Lumsden AB. Incidence and characteristics of patients with hand ischemia after a hemodialysis access procedure. J Surg Res 1998;74:8–10.
Rutherford RB. The value of noninvasive testing before and after hemodialysis access in the prevention and management of complications. Semin Vasc Surg 1997;10:157–161.
Thermann F, Brauckhoff M, Kornhuber M. Dialysis shuntassociated ischaemic monomelic neuropathy: neurological recovery preserving the dialysis access. Nephrol Dial Transplant 2006;21:3334–3336 (16854852).
Tordoir JHM, Dammers R, van der Sande FM. Upper extremity ischemia and hemodialysis vascular access. Eur J Vasc Endovasc Surg 2004;27:1–5.
van Gemert MJ, Bruyninckx CM. Simulated hemodynamic comparison of arteriovenous fistulas. J Vasc Surg 1987;6:39–44.
Wodicka R, Isaacs J. Ischemic monomelic neuropathy. J Hand Surg Am 2010;35:842e3 (19942360).
Yeager RA, Moneta GL, Edwards JM et al. Relationship of hemodialysis access to finger gangrene in patients with end-stage renal disease. J Vasc Surg 2002;36:245–249.
19.2. Предлагаем направить терапевтическое лечение на усиление артериального притока, уменьшение потока в доступе и/или дистальную реваскуляризацию. Когда вышеперечисленные методы не приносят улучшения, необходимо лигировать доступ.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. Активная ранняя хирургическая тактика предотвращает развитие и возникновение гангрены или необходимость ампутации.
Aschwanden M, Hess P, Labs KH, Dickenmann M, Jaeger KA. Dialysis access-associated steal syndrome: the intraoperative use of duplex ultrasound scan. J Vasc Surg 2003;37:211–213.
Balaji S, Evans JM, Roberts DE, Gibbons CP. Treatment of steal syndrome complicating a proximal arteriovenous bridge graft fistula by simple distal artery ligation without revascularization using intraoperative pressure measurements. Ann Vasc Surg 2003;17:320–322.
Berman SS, Gentile AT, Glickman MH et al. Distal revascularization-interval ligation for limb salvage and maintenance of dialysis access in ischemic steal syndrome. J Vasc Surg 1997;26:393–402.
DeCaprio JD, Valentine RJ, Kakish HB, Awad R, Hagino RT, Clagett GP. Steal syndrome complicating hemodialysis access. Cardiovasc Surg 1997;5:648–653.
Diehl L, Johansen K, Watson J. Operative management of distal ischemia complicating upper extremity dialysis access. Am J Surg 2003;186:17–19.
Ebeid A, Saranchak HJ. Banding of a PTFE hemodialysis fistula in the treatment of steal syndrome. Clin Exp Dial Apheresis 1981;5:251–257.
Goff CD, Sato DT, Bloch PH et al. Steal syndrome complicating hemodialysis access procedures: can it be predicted? Ann Vasc Surg 2000;14:138–144.
Gradman WS, Pozrikidis C. Analysis of options for mitigating hemodialysis access-related ischemic steal phenomena. Ann Vasc Surg 2004;18:59–65.
Guerra A, Raynaud A, Beyssen B, Pagny JY, Sapoval M, Angel C. Arterial percutaneous angioplasty in upper limbs with vascular access devices. Nephrol Dial Transplant 2002;17/5:843–851.
Haimov M, Schanzer H, Skladani M. Pathogenesis and management of upper-extremity ischemia following angioaccess surgery. Blood Purif 1996;14:350–354.
Katz S, Kohl RD. The treatment of hand ischemia by arterial ligation and upper extremity bypass after angioaccess surgery. J Am Coll Surg 1996;183:239–242.
Knox RC, Berman SS, Hughes JD, Gentile AT, Mills JL. Distal revascularization-interval ligation: a durable and effective treatment for ischemic steal syndrome after hemodialysis access. J Vasc Surg 2002;36:250–255.
Mattson WJ. Recognition and treatment of vascular steal secondary to hemodialysis prostheses. Am J Surg 1987;154:198–201.
Odland MD, Kelly PH, Ney AL, Andersen RC, Bubrick MP. Management of dialysis-associated steal syndrome complicating upper extremity arteriovenous fistulas: use of intraoperative digital photoplethysmography. Surgery 1991;110:664–669.
Papasavas PK, Reifsnyder T, Birdas TJ, Caushaj PF, Leers S. Prediction of arteriovenous access steal syndrome utilizing digital pressure measurements. Vasc Endovasc 2003;37:179–184.
Schanzer H, Skladany M, Haimov M. Treatment of angioaccessinduced ischemia by revascularization. J Vasc Surg 1992;16:861–864.
Sessa C, Riehl G, Porcu P et al. Treatment of hand ischemia following angioaccess surgery using the distal revascularization interval-ligation technique with preservation of vascular access: description of an 18-Case Series. Ann Vasc Surg 2004;18;685–694.
Shemesh D, Mabjeesh NJ, Abramowitz HB. Management of dialysis access-associated steal syndrome: use of intraoperative duplex ultrasound scanning for optimal flow reduction. J Vasc Surg 1999;30:193–195.
Stierli P, Blumberg A, Pfister J, Zehnder C. Surgical treatment of ‘steal syndrome’ induced by arteriovenous grafts for hemodialysis. J Cardiovasc Surg 1998;39:441–443.
Trerotola SO, Shah H, Johnson MS, Namyslowski J, Moresco KP, Patel NH. Hemodialysis graft: use as access for upper and lower extremity arteriography and interventional procedures – initial experience. Radiology 1999; 213:301–302.
Valentine RJ, Bouch ChW, Scott DJ, et al. Do preoperative finger pressures predict early arterial steal in hemodialysis access patients? A prospective analysis. J Vasc Surg 2002;36:351–356.
Valji K, Hye RJ, Roberts AC, Oglevie SB, Ziegler T, Bookstein JJ. Hand ischemia in patients with hemodialysis access grafts: angiographic diagnosis and treatment. Radiology 1995;196:697–701.
Zanow J, Kruger U, Scholz H. Proximalization of the arterial inflow: a new technique to treat access-related ischemia. J Vasc Surg 2006 Jun;43(6):1216–1221.
Комментарии. Для ранней, критической, угрожающей жизни ишемии, индуцированной сосудистым доступом, и для всех случаев ранней ишемической мономелической невропатии в отсутствие стил-синдрома АВ-доступ должен быть срочно лигирован.
Aimaq R, Katz SG. Using distal revascularization with interval ligation as the primary treatment of hand ischemia after dialysis access creation. J Vasc Surg 2013;57:1073–1078 (discussion 8).
Miles AM. Upper limb ischemia after vascular access surgery: differential diagnosis and management. Semin Dial 2000;13:312–325.
Padberg Jr FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg 2008;48:55S–80S.
Thermann F, Brauckhoff M, Kornhuber M. Dialysis shuntassociated ischaemic monomelic neuropathy: neurological recovery preserving the dialysis access. Nephrol Dial Transplant 2006;21:3334–3336 (16854852).
Thermann F, Kornhuber M. Ischemic monomelic neuropathy: a rare but important complication after hemodialysis access placementea review. J Vasc Access 2011;12:113–119 (21360465).
Комментарии. У пациентов с клиническими признаками крайней степени ишемии конечностей с индуцированным стенозом артериального притока сосудистого доступа возможна баллонная ангиопластика как вариант лечения.
Guerra A, Raynaud A, Beyssen B, Pagny JY, Sapoval M, Angel C. Arterial percutaneous angioplasty in upper limbs with vascular access devices for haemodialysis. Nephrol Dial Transplant 2002;17:843–851.
Malik J, Tuka V, Kasalova Z, Chytilova E, Slavikova M, Clagett P, et al. Understanding the dialysis access steal syndrome. A review of the etiologies, diagnosis, prevention and treatment strategies. J Vasc Access 2008;9:155-66.
Комментарии. Пациентам с клиническими признаками крайней степени ишемии конечностей и с высоким потоком в сосудистом доступе следует выполнять хирургическое вмешательство, направленное на уменьшение потока в доступе.
Callaghan CJ, Mallik M, Sivaprakasam R, Iype S, Pettigrew GJ. Treatment of dialysis access-associated steal syndrome with the “revision using distal inflow” technique. J Vasc Access 2011;12:52–56.
Mickley V. Steal syndromeestrategies to preserve vascular access and extremity. Nephrol Dial Transplant 2008;23:19–24.
Комментарии. Пациентам с индуцированным сосудистым доступом ишемией конечности и без высокого кровотока в доступе на плече показана дистальная реваскуляризация и временная перевязка доступа.
Al Shakarchi J, Stolba J, Houston JG, Inston N. Surgical techniques for haemodialysis access-induced distal ischaemia. J Vasc Access 2016;17:40–46.
Anaya-Ayala JE, Pettigrew CD, Ismail N, Diez-De Sollano AL, Syed FA, Ahmed FG, et al. Management of dialysis accessassociated “steal” syndrome with DRIL procedure: challenges and clinical outcomes. J Vasc Access 2012;13:299–304.
Field M, Blackwell J, Jaipersad A,Wall M, Silva MA, Morgan RH, et al. Distal revascularisation with interval ligation (DRIL): an experience. Ann R Coll Surg Engl 2009;91:394–398.
Gupta N, Yuo TH, Konig G, Dillavou E, Leers SA, Chaer RA, et al. Treatment strategies of arterial steal after arteriovenous access. J Vasc Surg 2011;54:162–167.
Knox RC, Berman SS, Hughes JD, Gentile AT, Mills JL. Distal revascularization-interval ligation: a durable and effective treatment for ischemic steal syndrome after hemodialysis access. J Vasc Surg 2002;36:250–255 (discussion 6).
Misskey J, Yang C, MacDonald S, Baxter K, Hsiang Y. A comparison of revision using distal inflow and distal revascularization-interval ligation for the management of severe access-related hand ischemia. J Vasc Surg 2016;63:1574–1581.
20. Инфекция АВ-доступа
Артериовенозные фистулы
20.1. При возникновении ранней периоперационной инфекции (<30 дней) пациентам с аутогенной АВ-фистулой в отсутствие кровотечений или псевдоаневризм рекомендуется соответствующая антибиотикотерапия.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Padberg Jr FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg 2008;48:55S–80S.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
20.2. При возникновении ранней периоперационной инфекции пациентам с аутогенной АВ-фистулой при наличии системных признаков воспаления, кровотечения и вовлечения в патологический процесс анастомоза необходимо лигировать АВ-доступ.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Padberg Jr FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: recognition and management. J Vasc Surg 2008;48:55S–80S.
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
Артериовенозные трансплантаты
20.3. При возникновении ранней периоперационной инфекции (<30 дней) пациентам с АВ-трансплантатом при наличии системным признаков сепсиса, гнойного выделения, абсцесса в месте локализации трансплантата или кровотечения следует удалить трансплантат.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Schmidli J, Widmer MK, Basile C et al. Vascular access: 2018 clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757–818.
20.4. Все поздние инфекции сосудистого доступа следует лечить антибиотиками для покрытия спектра как грамположительных, так и грамотрицательных микроорганизмов.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Kessler M, Hoen B, Mayeux D, Hestin D, Fontenaille C. Bacteremia in patients on chronic hemodialysis. A multicenter prospective survey. Nephron 1993;64:95–100.
Lentino JR, Baddour LM, Wray M, Wong ES, Yu VL. Staphylococcus aureus and other bacteremias in hemodialysis patients: antibiotic therapy and surgical removal of access site. Infection 2000;28:355–360.
20.5. При поздней инфекции АВ-трансплантата рекомендуется удаление трансплантата у пациентов с сепсисом, клиническими признаками инфекции и наличием жидкости вокруг него.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Ryan SV, Calligaro KD, Dougherty MJ. Management of hemodialysis access infections. Semin Vasc Surg 2004;17:40–44.
Schutte WP, Helmer SD, Salazar L, Smith JL. Surgical treatment of infected prosthetic dialysis arteriovenous grafts: total versus partial graft excision. Am J Surg 2007;193:385–38. discussion 8.
Schwab DP, Taylor SM, Cull DL, Langan 3rd EM, Snyder BA, Sullivan TM, et al. Isolated arteriovenous dialysis access graft segment infection: the results of segmental bypass and partial graft excision. Ann Vasc Surg 2000;14:
63–66.
21. Аневризма АВ-доступа
21.1. Рекомендуется хирургическое вмешательство для ревизии аневризм АВ-доступа, если места канюлирования и диаметр доступа могут быть сохранены.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Georgiadis GS, Lazarides MK, Panagoutsos SA, Kantartzi KM, Lambidis CD, Staramos DN, et al. Surgical revision of complicated false and true vascular access-related aneurysms. J Vasc Surg 2008;47:1284–1291.
Spergel LM, Ravani P, Roy-Chaudhury P, Asif A, Besarab A. Surgical salvage of the autogenous arteriovenous fistula (AVF). J Nephrol 2007;20:388–398.
21.2. Рекомендуется хирургическое вмешательство для ревизии псевдоаневризм в АВ-трансплантатах, если они ограничивают доступность места канюлирования, ассоциируются с болью, плохим образованием рубцов, спонтанным кровотечением и патологическим расширением.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Georgiadis GS, Lazarides MK, Panagoutsos SA, Kantartzi KM, Lambidis CD, Staramos DN, et al. Surgical revision of complicated false and true vascular access-related aneurysms. J Vasc Surg 2008;47:1284–1291.
Shemesh D, Goldin I, Zaghal I, Berelowitz D, Verstandig AG, Olsha O. Stent graft treatment for hemodialysis access aneurysms. J Vasc Surg 2011;54:1088–1094.
21.3. Канюляции доступа через псевдоаневризмы не рекомендуется.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Charara J, Guidoin R, Gill F, Guzman R. Morphologic assessment of ePTFE graft wall damage following hemodialysis needle punctures. J Appl Biomater 1990;1:279–287.
Delorme JM, Guidoin R, Canizales S, Charara J, How T, Marois Y, et al. Vascular access for hemodialysis: pathologic features of surgically excised ePTFE grafts. Ann Vasc Surg 1992;6:517–524.
21.4. При симптоматических аневризмах сосудистого доступа должен быть исключен стеноз оттока, при их наличии – лечиться.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Pandolfe LR, Malamis AP, Pierce K, Borge MA. Treatment of hemodialysis graft pseudoaneurysms with stent grafts: institutional experience and review of the literature. Semin Intervent Radiol 2009;26:89–95.
Shah AS, Valdes J, Charlton-Ouw KM, Chen Z, Coogan SM, Amer HM, et al. Endovascular treatment of hemodialysis access pseudoaneurysms. J Vasc Surg 2012;55:1058–1062.
Spergel LM, Ravani P, Roy-Chaudhury P, Asif A, Besarab A. Surgical salvage of the autogenous arteriovenous fistula (AVF). J Nephrol 2007;20:388–398.
22. Закрытие АВ-доступа
22.1. Рутинного закрытия функционирующего сосудистого доступа после успешной трансплантации почки не рекомендуется.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Soleimani MJ, Shahrokh H, Shadpour P, Shirani M, Arasteh S. Impact of dialysis access fistula on cardiac function after kidney transplantation. Iran J Kidney Dis 2012;6:198–202.
22.2. Закрытие сосудистого доступа следует рассматривать у пациентов с рефрактерной сердечной недостаточностью после трансплантации.
Уровень достоверности доказательств IV, уровень убедительности рекомендаций C
Cridlig J, Selton-Suty C, Alla F, Chodek A, Pruna A, Kessler M, et al. Cardiac impact of the arteriovenous fistula after kidney transplantation: a case-controlled, match-paired study. Transpl Int 2008;21:948–954.
Soleimani MJ, Shahrokh H, Shadpour P, Shirani M, Arasteh S. Impact of dialysis access fistula on cardiac function after kidney transplantation. Iran J Kidney Dis 2012;6:198–202.
Unger P, Wissing KM, de Pauw L, Neubauer J, van de Borne P. Reduction of left ventricular diameter and mass after surgical arteriovenous fistula closure in renal transplant recipients. Transplantation 2002;74:73–79.
van Duijnhoven EC, Cheriex EC, Tordoir JH, Kooman JP, van Hooff JP. Effect of closure of the arteriovenous fistula on left ventricular dimensions in renal transplant patients. Nephrol Dial Transplant 2001;16:368–372.
ЦЕНТРАЛЬНЫЙ ВЕНОЗНЫЙ КАТЕТЕР ДЛЯ ДИАЛИЗА
1. Концепция использования центральных венозных катетеров для диализа
1.1. Полагаем, что центральные венозные катетеры для гемодиализа должны использоваться только для диализа или подобных экстракорпоральных процедур для взрослых пациентов.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. Врач объясняет пациенту (если это возможно) или его законному представителю особенности процедуры катетеризации, возможные осложнения и причины, по которым необходимо введение катетера. Врач, установивший ЦВК, оформляет медицинскую документацию. Запись должна включать показания (предписание) к катетеризации; дату и время введения ЦВК; тип катетера, его размер (G/Fr), длину катетера; анатомическую область места доступа; антисептик, использованный для хирургической обработки операционного поля; анестетик; наличие и характер осложнений или их отсутствие при катетеризации; дополнительные рекомендации по уходу за катетером; данные врача, осуществившего постановку катетера, и его подпись.
Al-Balas A, Lee T,Young CJ,Kepes JA,Barker-Finkel J, Allon M: The clinical and economic effect of vascular access selection in patients initiating hemodialysis with a catheter. J AmSoc Nephrol 28: 3679–3687, 2017.
Dugue´ AE, Levesque SP, Fischer MO, Souweine B, Mira JP, Megarbane B, et al. Vascular access sites for acute renal replacement in intensive care units. Clin J Am Soc Nephrol CJASN 2012;7:70–77.
Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
Hoste EAJ, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med 2015;41:1411–1423.
Jindal K, Chan CT, Deziel C et al. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. Chapter 4: vascular access. J Am Soc Nephrol 2006;17(Suppl 1):S16–S23.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012;120:179–184.
Mermel LA. Prevention of intravascular catheter-related infections. Ann Intern Med 2000;132:391–402.
National Kidney Foundation. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for 2006 updates: hemo‐ dialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis. 2006;48(Suppl 1):S1–S322.
Polkinghorne K, Dent H, Gulyani A et al, Haemodialysis in ANZDATA Thirty Fourth Annual Report. 2011, Australia and New Zealand Dialysis and Transplant Registry: Adelaide, South Australia. Р. 5–25, 5–31.
Polkinghorne KR, Chin GK, MacGinley RJ, et al. KHA-CARI guideline: vascular access—central venous catheters, arteriovenous fistulae, and arteriovenous grafts. Nephrology. 2013;18:701–705.
Rayner HC, Besarab A, Brown WW, Disney A, Saito A, Pisoni RL. Vascular access results from the Dialysis Outcomes and Practice Patterns Study (DOPPS): performance against Kidney Disease Outcomes Quality Initiative (K/DOQI) Clinical Practice Guidelines. Am J Kidney Dis 2004;44:22–26.
Rayner HC, Pisoni RL. The increasing use of hemodialysis catheters: evidence from the DOPPS on its significance and ways to reverse it. Semin Dial. 2010;23:6.
Tordoir J, Canaud B, Haage P et al. EBPG on Vascular Access. Nephrology Dialysis Transplantation. 2007; 22: ii88–117.
1.2. Предлагаем использовать нетуннелированный катетер для гемодиализа, когда не требуется длительного лечения, при необходимости оказания экстренной или неотложной помощи методами экстракорпорального диализа взрослым пациентам при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Нетуннелированный катетер часто требуется в качестве доступа для гемодиализа взрослым пациентам при состояниях при ХБП-5, без постоянного доступа, когда продолжительность диализа, которая потребуется, не может быть легко предсказана. Использование нетуннелированных катетеров как доступа для экстракорпорального диализ должно быть ограничено семью днями при локализации во внутренней яремной вене или подключичной и максимум пятью днями на бедре.
Filiopoulos V, Hadjiyannakos D, Koutis I et al. Approaches to prolong the use of uncuffed hemodialysis catheters: results of a randomized trial. Am J Nephrol 2011;33:260–268.
Merrer J, De JB, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. Jama. 2001; 286(6):700–707. [PubMed: 11495620].
Parienti JJ, du Cheyron D, Timsit JF, et al. Meta-analysis of subclavian insertion and nontunneled central venous catheter–associated infection risk reduction in critically ill adults. Crit Care Med 2012;40(5):1627–1634.
Allon M: Current management of vascular access. Clin J Am Soc Nephrol 2:786–800, 2007.
Bagshaw SM, Mortis G, Godinez-Luna T et al. Renal recovery after severe acute renal failure. Int J Artif Organs 2006;29:1023–1030.
Bay WH, Van Cleef S, Owens M. The hemodialysis access: preferences and concerns of patients, dialysis nurses and technicians, and physicians. Am J Nephrol 1998;18:379–383.
Canaud B, Desmeules S. Vascular access for hemodialysis. In: Ho¨rl W, Koch KM, Lindsay RM, Ronco C, Winchester JF, eds. Replacement of Renal Function by Dialysis, 5th edn, Kluwer Academic Publishers, London: 2004;9:203–230.
Collins AJ, Foley RN, Gilbertson DT, Chen SC: The state of chronic kidney disease, ESRD, and morbidity and mortality in the first year of dialysis. Clin J Am Soc Nephrol 4[Suppl 1]:S5–S11, 2009.
Trerotola SO, Shah H, Johnson M et al. Randomized comparison of high-flow versus conventional hemodialysis catheters. J Vasc Interv Radiol 1999;10:1032–1038.
Vats HS: Complications of catheters: Tunneled and nontunneled. Adv Chronic Kidney Dis 19:188–194, 2012.
1.3. Предлагаем использовать стандартный центральный венозный двупросветный нетуннелированный катетер для гемодиализа в качестве сосудистого доступа для начала лечения методами экстракорпорального диализа взрослых пациентов при критических состояниях и при остром повреждении почек.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Затраты и условия не оправдывают трудностей, связанных с установкой туннелированных катетеров в качестве первого сосудистого доступа всем больным ОПП, для начала лечения методами экстракорпорального диализа. Однако в настоящее время обоснована избирательная установка туннелированных катетеров больным, нуждающимся в длительной медицинской помощи методами диализа. Рекомендаций по оптимальным срокам замены нетуннелированных безманжеточных катетеров на более постоянный доступ при ОПП не существует в настоящее время.
Klouche K, Amigues L, Deleuze S, et al. Complications, effects on dialysis dose, and survival of tunneled femoral dialysis catheters in acute renal failure. Am J Kidney Dis 2007;49:99–108.
Oliver MJ, Edwards LJ, Treleaven DJ, et al. Randomized study of temporary hemodialysis catheters. Int J Artif Organs 2002;25:40–44.
Parienti JJ, Megarbane B, Fischer MO, et al. Catheter dysfunction and dialysis performance according to vascular access among 736 critically ill adults requiring renal replacement therapy: a randomized controlled study. Crit Care Med 2010;38:1118–1125.
1.4. Предлагаем использовать туннелированный катетер для гемодиализа, если ожидается, что сосудистый доступ будет востребован более 3 недель, в том числе если не ожидается или ожидается отсроченное восстановление функции почек, при необходимости оказания неотложной помощи методами экстракорпорального диализа взрослым пациентам при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Доля пациентов, использующих туннелированный катетер как жизненно важную опцию, продолжает оставаться повсеместно высокой с преобладающим использованием взрослыми пациентами при состояниях при ХБП-5, начинающими получать медицинскую помощь методами диализа. Отчасти это может быть объяснено недостаточно отрегулированным планирования начала диализа, отсутствием додиализного наблюдения нефрологом, тяжелыми сопутствующими заболеваниями и ограниченностью продолжительности жизни и/или из-за анатомии сосудов.
Canaud B, Leray-Moragues H, Kerkeni N, Bosc JY, Martin K. Effective flow performances and dialysis doses delivered with permanent catheters: a 24-month comparative study of permanent catheters versus arterio-venous vascular accesses. Nephrol Dial Transpl 2002;17:1286–129.2
Edward G. Clark Jeffrey H. Barsuk. Temporary hemodialysis catheters: recent advances Kidney International (2014) 86, 888–895; doi:10.1038/ki.2014.162;
Flowers RH 3rd, Schwenzer KJ, Kopel RF, Fisch MJ, Tucker SI, Farr BM. Efficacy of an attachable subcutaneous cuff for the prevention of intravascular catheter-related infection A randomized, controlled trial. JAMA. 1989; 261(6):878–883. [PubMed: 2492354] J Vasc Access. 2012;13:51–54.
Flowers RH 3rd, Schwenzer KJ, Kopel RF, Fisch MJ, Tucker SI, Farr BM. Efficacy of an attachable subcutaneous cuff for the prevention of intravascular catheter-related infection A randomized, controlled trial. JAMA. 1989; 261(6):878–883. [PubMed: 2492354] J Vasc Access. 2012;13:51–54.
Ge X, Cavallazzi R, Li C et al. Central venous access sites for the prevention of venous thrombosis, stenosis and infection. Cochrane Database of Systematic Reviews. 2012: Art.No.:CD004084 DOI:10.1002/14651858.CD004048.pub3.
Lee T.: Tunneled catheters in hemodialysis patients: Reasons and subsequent outcomes. AmJ Kidney Dis 46: – 501–508,2005.
Little MA, O’Riordan A, Lucey B et al. A prospective study of complications associated with cuffed, tunneled haemodialysis catheters. Nephrol. Dial. Transplant. 2001;16:2194–200.
Mokrzycki MH, Singhal A. Cost-effectiveness of three strategies of managing tunnelled, cuffed haemodialysis catheters in clinically mild or asymptomatic bacteraemias. Nephrol Dial Transplant 2002;17:2196–2203:135.
Ori Y, Korzets A, Katz M et al. The contribution of an arteriovenous access for hemodialysis to left ventricular hypertrophy. Am J Kidney Dis 2002;40:745–752.
Perl J, Wald R, McFarlane P, Bargman JM, Vonesh E, Na Y, et al. Hemodialysis vascular access modifies the association between dialysis modality and survival. J Am Soc Nephrol 2011;22:1113–1121.
Poinen K, Quinn RR, Clarke A, et al. Complications from tunneled hemodialysis catheters: a Canadian observational cohort study. Am J Kidney Dis. 2019;73(4):467–-475.
Polkinghorne KR, McDonald SP, Atkins RC, Kerr PG. Vascular access and all-cause mortality: a propensity score analysis. J Am Soc Nephrol 2004;15:477–486.
Wang H, Huang T, Jing J, et al. Effectiveness of different central venous catheters for catheter-related infections: a network meta-analysis. J Hosp Infect 2010;76(1):1–11.
1.5. Полагаем, что туннелированные катетеры для гемодиализа ассоциируются с более низкой частотой инфекции кровотока, дисфункции катетера и сосудистых повреждений (травма вены и стеноз) у взрослых пациентов при состояниях при ХБП-5 по сравнению с временными нетуннелированными катетерами для гемодиализа.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. В настоящее время невозможно дать рекомендации в отношении предпочтительного места локализации для туннелированного ЦВК, чтобы свести к минимуму риск инфицирования.
Clark EG, Barsuk JH2.Temporary hemodialysis catheters: recent advances. Kidney Int. 2014 Nov;86(5):888–895. Doi: 10.1038/ki.2014.162. Epub 2014 May 7.
Flowers RH 3rd, Schwenzer KJ, Kopel RF, Fisch MJ, Tucker SI, Farr BM. Efficacy of an attachable subcutaneous cuff for the prevention of intravascular catheter-related infection A randomized, controlled trial. JAMA. 1989; 261(6):878–883. [PubMed: 2492354] J Vasc Access. 2012;13:51–54.
Ge X, Cavallazzi R, Li C et al. Central venous access sites for the prevention of venous thrombosis, stenosis and infection. Cochrane Database of Systematic Reviews. 2012: Art.No.:CD004084. Doi: 10.1002/14651858.CD004048.pub3.
Little MA, O’Riordan A, Lucey B et al. A prospective study of complications associated with cuffed, tunneled haemodialysis catheters. Nephrol. Dial. Transplant. 2001;16:2194–200.
Mokrzycki MH, Singhal A. Cost-effectiveness of three strategies of managing tunnelled, cuffed haemodialysis catheters in clinically mild or asymptomatic bacteraemias. Nephrol Dial Transplant 2002;17:2196–2203:135.
Nagashima G, Kikuchi T, Tsuyuzaki H et al. To reduce catheter-related bloodstream infections: is the subclavian route better than the jugular route for central venous catheterization? Journal of Infection & Chemotherapy. 2006;12:363–365.
Oguzkurt L, Tercan F, Torun D et al. Impact of short-term hemodialysis catheters on the central veins: a catheter venographic study. European Journal of Radiology. 2004;52:293–299.
Poinen K, Quinn RR, Clarke A, et al. Complications from tunneled hemodialysis catheters: a Canadian observational cohort study. Am J Kidney Dis. 2019;73(4):467–475.
Taal MW, Chesterton LJ, and McIntyre CW. Venography at insertion of tunnelled internal jugular vein dialysis catheters reveals significant occult stenosis. Nephrology Dialysis Transplantation. 2004;19:1542–1545.
Thomson P, Stirling C, Traynor J et al. A prospective observational study of catheter-related bacteraemia and thrombosis in a haemodialysis cohort: univariate and multivariate analyses of risk association. Nephrology Dialysis Transplantation. 2010;25:1596–1604.
Weijmer MC, Vervloet MG, and ter Wee PM. Compared to tunnelled cuffed haemodialysis catheters, temporary untunnelled catheters are associated with more complications already within 2 weeks of use. Nephrology Dialysis Transplantation. 2004;19:670–677.
Wang H, Huang T, Jing J, et al. Effectiveness of different central venous catheters for catheter-related infections: a network meta-analysis. J Hosp Infect 2010;76(1):1–11.
Marik PE, Flemmer M, HarrisonW. The risk of catheter-related bloodstream infection with femoral venous catheters as compared to subclavian and internal jugular venous catheters: a systematic review of the literature and meta-analysis. Crit Care Med 2012;40(8):2479–2485.
Oliver MJ, Callery SM, Thorpe KE et al. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: a prospective study. Kidney Int 2000;58:2543–2545.
Wilkin TD: Internal jugular vein thrombosis associated with hemodialysis catheters. Radiology 228: 697–700, 2003.
Thomson P, Stirling C, Traynor J, Morris S, Mactier R. A prospective observational study of catheter-related bacteraemia and thrombosis in a haemodialysis cohort: univariate and multivariate analyses of risk associations. Nephrol Dial Transplant 2010; 25(5):1596–1560.
1.6. Рекомендуем информировать медицинский персонал, осуществляющий формирование сосудистого доступа для диализа, о базовом перечне катетеров для гемодиализа, что позволит выбрать наиболее подходящий тип катетера, его размер (G/Fr), длину катетера, исходя из конституционных особенностей и клинического состояния пациента.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Медицинский персонал, который осуществляет формирование доступа, учитывает материал, из которого сделан катетер, и количество просветов в нем, анатомическую область места доступа, длительность лечения методами диализа, риски осложнений, включая инфекционные, требования к положению дистального участка катетера и иные индивидуальные особенности пациента.
Agarwal AK, Ash SR. Maintenance of blood flow rate on dialysis with selfcentering Centros-FLO catheter: a multicenter prospective study. Hemodial Int. 2016;20:501–509.
Almasri J, Alsawas M, Mainou M, et al. Outcomes of vascular access for hemodialysis: a systematic review and meta-analysis. J Vasc Surg. 2016;64(1):236–243.
Appelgren P, Ransjö U, Bindslev L, Espersen F, Larm O. Surface heparinization of central venous catheters reduces microbial colonization in vitro and in vivo: results from a prospective, randomized trial. Crit Care Med. 1996 Sep;24(9):1482–1489.
Dwyer A. Surface-treated catheters--a systematic review. Semin Dial. 2008 Nov-Dec;21(6):542–546. Doi: 10.1111/j.1525-139X 2008.00499.x. Epub 2008 Sep 24.
Filiopoulos V, Hadjiyannakos D, Koutis I et al. Approaches to prolong the use of uncuffed hemodialysis catheters: results of a randomized trial. Am J Nephrol 2011;33:260–268.
Flowers RH 3rd, Schwenzer KJ, Kopel RF, Fisch MJ, Tucker SI, Farr BM. Efficacy of an attachable subcutaneous cuff for the prevention of intravascular catheter-related infection A randomized, controlled trial. JAMA. 1989;261(6):878–883. [PubMed: 2492354]. J Vasc Access. 2012;13:51–54.
Gallieni M, Brenna I, Brunini F, et al. Dialysis central venous catheter types and performance. J Vasc Access. 2014;15(suppl 7):S140–S146.
Gilbert RE, Harden M. Effectiveness of impregnated central venous catheters for catheter related blood stream infection: a systematic review. Curr Opin Infect Dis. 2008;21:235–245.
Hwang HS, Kang SH, Choi SR, Sun IO, Park HS, Kim Y. Comparison of the palindrome vs. step-tip tunneled hemodialysis catheter: a prospective randomized trial: comparison of the palindrome vs. step-tip catheter. Semin Dial 2012;25:587–591.
Leblanc M, Fedak S, Mokris G, et al. Blood recirculation in temporary central catheters for acute hemodialysis. Clin Nephrol 1996;45:315–319.
Little MA, Conlon PJ, Walshe JJ. Access recirculation in temporary hemodialysis catheters as measured by the saline dilution technique. Am J Kidney Dis 2000;36:1135–1139.
Maki DG, Stolz SM, Wheeler S, Mermel LA Prevention of central venous catheter-related bloodstream infection by use of an antiseptic-impregnated catheter. A randomized, controlled trial. Ann Intern Med. 1997 Aug 15;127(4):257–266.
Marik PE, Flemmer M, HarrisonW. The risk of catheter-related bloodstream infection with femoral venous catheters as compared to subclavian and internal jugular venous catheters: a systematic review of the literature and meta-analysis. Crit Care Med 2012;40(8):2479–2485
Merrer J, De JB, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. Jama. 2001;286(6):700–707. [PubMed: 11495620].
Moossavi S, Vachharajani TJ, Jordan J, Russell GB, Kaufman T, Moossavi S: Retrospective analysis of catheter recirculation in prevalent dialysis patients. Semin Dial 21:289–292, 2008.
Morgan D, Ho K, Murray C, Davies H, Louw J. A randomized trial of catheters of different lengths to achieve right atrium versus superior vena cava placement for continuous renal replacement therapy. Am J Kidney Dis 2012;60:272–279.
Oliver MJ. Acute dialysis catheters. Semin Dial 2001;14:432–435.
Parienti JJ, Thirion M, Megarbane B, et al. Femoral vs jugular venous catheterization and risk of nosocomial events in adults requiring acute renal replacement therapy: a randomized controlled trial. Jama. 2008; 299(20):2413–2422. [PubMed: 18505951].
Ravani P, Palmer SC, Oliver MJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol: JASN. 2013;24(3):465-473.
Rosenblum A, WangW, Ball LK, Latham C,MadduxFW, Lacson E Jr.: Hemodialysis catheter care strategies: A cluster-randomized quality improvement initiative. Am J Kidney Dis 63: 259–267, 2014.
Ruesch S, Walder B, Tramer MR. Complications of central venous catheters: internal jugular versus subclavian access--a systematic review. Crit Care Med. 2002;30(2):454–460. [PubMed: 11889329].
Rupp ME, Lisco SJ, Lipsett PA, Perl TM, Keating K, Civetta JM, Mermel LA, Lee D, Dellinger EP, Donahoe M, Giles D, Pfaller MA, Maki DG, Sherertz R Effect of a second-generation venous catheter impregnated with chlorhexidine and silver sulfadiazine on central catheter-related infections: a randomized, controlled trial. Ann Intern Med. 2005 Oct 18;143(8):570–580.
Schindler R, Heemann U, Haug U et al. Bismuth coating of non-tunneled haemodialysis catheters reduces bacterial colonization: a randomized controlled trial. Nephrol Dial Transplant 2010;25:2651–2656.
Trerotola SO, Johnson MS, Shah H, et al. Tunneled hemodialysis catheters: use of a silver coated catheter for prevention of infection – a randomized study. Radiology. 1998;207:491–496.
Trerotola SO, Kraus M, Shah H, Namyslowski J, Johnson MS, SteckerMS, Ahmad I, McLennan G, Patel NH, O’Brien E, Lane KA, AmbrosiusWT. Randomized comparison of splittip versus steptip high-flow hemodialysis catheters. Kidney Int 62:282–289, 2002.
Trivedi HS, Vachharajani TJ, Wadhwa N, et al. Multicenter randomized study comparing symmetric tip versus split tip dialysis tunneled catheter. Poster presented at: American Society of Nephrology Kidney Week 2014. November 11–16, 2014; Philadelphia, PA.
Trottier SJ, Veremakis C, O'Brien J, Auer AI. Femoral deep vein thrombosis associated with central venous catheterization: results from a prospective, randomized trial. Crit Care Med. 1995;23(1):52–59. [PubMed: 8001386].
Van Der Meersch H, De Bacquer D, Vandecasteele SJ, et al. Hemodialysis catheter design and catheter performance: a randomized controlled trial. Am J Kidney Dis. 2014;64:902–908.
Veenstra DL, Saint S, Saha S et al. Efficacy of antiseptic-impregnated central venous catheters in preventing catheter-related bloodstream infection: a meta-analysis. JAMA. 1999;281:261–267.
Wang H, Huang T, Jing J, et al. Effectiveness of different central venous catheters for catheter-related infections: a network meta-analysis. J Hosp Infect 2010;76(1):1–11.
1.7. Полагаем, что правая внутренняя яремная вена является предпочтительным местом для введения туннелированного катетера для гемодиализа с более низкой частотой краткосрочных и долгосрочных осложнений у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций B
Комментарии. Катетеры, вставленные в правую внутреннюю яремную вену, обеспечивают лучший кровоток по сравнению с другими локализациями ЦВК для диализа, лучшую выживаемость доступа по сравнению с левосторонней локализацией внутренней яремной вены и бедренной локализацией. В силу индивидуальных особенностей пациента порядок данной предпочитаемой последовательности может быть изменен.
Agarwal AK, Ash SR; Principal Investigators of the Centros FLO Trial: Maintenance of blood flow rate on dialysis with selfcentering Centros FLO catheter: A multicenter prospective study. Hemodial Int 20:501–509, 2016.
Agarwal AK, Patel BM, Haddad NJ. Central vein stenosis: a nephrologist’s perspective. Semin Dial 2007;20:53–62.
Balamuthusamy S: Self-centering, split-tip catheter has better patency than symmetric-tip tunneled hemodialysis catheter: Single-center retrospective analysis. Semin Dial 27:522–528, 2014.
Dugue AE, Levesque SP, Fischer MO et al. Vascular access sites for acute renal replacement in intensive care units. Clin J Am Soc Nephrol 2012;7:70–77.
Engstrom BI, Horvath JJ, Stewart JK, et al. Tunneled internal jugular hemodialysis catheters: impact of laterality and tip position on catheter dysfunction and infection rates. J Vasc Interv Radiol: JVIR. 2013;24(9):1295–1302.
Fry AC, Stratton J, Farrington K et al. Factors affecting long-term survival of tunnelled haemodialysis catheters--a prospective audit of 812 tunnelled catheters. Nephrology Dialysis Transplantation. 2008;23:275–281.
Jean G, Charra B, Chazot C, Vanel T, Terrat JC, Hurot JM. Long-term outcome of permanent hemodialysis catheters: a controlled study. Blood Purif 2001;19:401–407.
Lorente L, Henry C, Martin MM, Jimenez A, Mora ML. Central venous catheter-related infection in a prospective and observational study of 2,595 catheters. Crit Care. 2005; 9(6):R631–R635. [PubMed: 16280064].
Marik PE, Flemmer M, HarrisonW. The risk of catheter-related bloodstream infection with femoral venous catheters as compared to subclavian and internal jugular venous catheters: a systematic review of the literature and meta-analysis. Crit Care Med 2012;40(8):2479–2485.
Mokrzycki MH, Lok CE. Traditional and non-traditional strategies to optimize catheter function: Go with more flow. Kidney Int 78:1218–1231, 2010.
Moossavi S, Vachharajani TJ, Jordan J, Russell GB, Kaufman T, Moossavi S: Retrospective analysis of catheter recirculation in prevalent dialysis patients. Semin Dial 21:289–292, 2008.
Morgan D, Ho K, Murray C, Davies H, Louw J. A randomized trial of catheters of different lengths to achieve right atrium versus superior vena cava placement for continuous renal replacement therapy. Am J Kidney Dis 2012;60:272–279.
Oguzkurt L, Tercan F, Torun D, et al. Impact of short-term hemodialysis catheters on the central veins: a catheter venographic study. Eur J Radiol 2004;52:293–299.
Oliver MJ, Callery SM, Thorpe KE et al. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: a prospective study. Kidney Int 2000;58:2543–2545.
Oliver MJ, Edwards LJ, Treleaven DJ, et al. Randomized study of temporary hemodialysis catheters. Int J Artif Organs 2002;25:40–44.
Ozyer U, Harman A, Yildirim E, Aytekin C, Karakayali F, Boyvat F. Long-term results of angioplasty and stent placement for treatment of central venous obstruction in 126 hemodialysis patients: a 10-year single-center experience. AJR Am J Roentgenol. 2009;193:1672–1679.
Parienti JJ, Megarbane B, Fischer MO et al. Catheter dysfunction and dialysis performance according to vascular access among 736 critically ill adults requiring renal replacement therapy: a randomized controlled study. Crit Care Med 2010;38:1118–1125.
Parienti JJ, Thirion M, Megarbane B, et al. Femoral vs jugular venous catheterization and risk of nosocomial events in adults requiring acute renal replacement therapy: a randomized controlled trial. Jama. 2008;299(20):2413–2422. [PubMed: 18505951].
Pisoni RL, Young EW, Dykstra DM, Greenwood RN, Hecking E, Gillespie B, Wolfe RA, Goodkin DA, Held PJ. Vascular access use in Europe and the United States: results from the DOPPS. Kidney Int. 2002 Jan;61(1):305–316.
Puel V, Caudry M, Le Metayer P, et al. Superior vena cava thrombosis related to catheter malposition in cancer chemotherapy given through implanted ports. Cancer 1993;72:2248–2252.
Ruesch S, Walder B, Tramer MR. Complications of central venous catheters: internal jugular versus subclavian access-a systematic review. Crit Care Med. 2002;30(2):454–460. [PubMed: 11889329].
Taal MW, Chesterton LJ, McIntyre CW. Venography at insertion of tunnelled internal jugular vein dialysis catheters reveals significant occult stenosis. Nephrol Dial Transplant 2004;19:1542–1545.
Thomson P, Stirling C, Traynor J, Morris S, Mactier R. A prospective observational study of catheter-related bacteraemia and thrombosis in a haemodialysis cohort: univariate and multivariate analyses of risk associations. Nephrol Dial Transplant 2010;25(5):1596–1660.
Vats HS, Bellingham J, Pinchot JW, Young HN, Chan MR, Yevzlin AS. A comparison between blood flow outcomes of tunneled external jugular and internal jugular hemodialysis catheters. J Vasc Access. 2012 Jan-Mar;13(1):51–54. Doi: 10.5301/JVA.2011.8444.
Wang H, Huang T, Jing J, et al. Effectiveness of different central venous catheters for catheter-related infections: a network meta-analysis. J Hosp Infect 2010;76(1):1–11.
Wilkin TD: Internal jugular vein thrombosis associated with hemodialysis catheters. Radiology, 228:697–700, 2003.
Yevzlin AS. Hemodialysis catheter-associated central venous stenosis. Semin Dial 2008; 21:522–527.
1.8. Мы рекомендуем по возможности всем избегать подключичной локализации катетера для гемодиализа, чтобы избежать стеноза подключичной вены у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. В условиях интенсивной терапии установка подключичного катетера имеет превосходные краткосрочные результаты по сравнению с яремным и бедренным доступами, но имеет значительные долгосрочные отрицательные последствия, если восстановление функции почек маловероятно, рекомендующие неиспользования этой локализации при оказании медицинской помощи методами диализа. Подключичный доступ следует рассматривать в последнюю очередь, когда варианты локализации во внутренней яремной вене недоступны. Если подключичная вена остается единственным доступом, предпочтение следует отдавать доминирующей руке, чтобы сохранить «нерабочую» руку для возможного формирования в последующем постоянного сосудистого доступа.
Agraharkar M, Isaacson S, Mendelssohn D et al. Percutaneously inserted silastic jugular hemodialysis catheters seldom cause jugular vein thrombosis. ASAIO Journal. 1995;41:169–172.
Babycos CR, Barrocas A, Webb WR. A prospective randomized trial comparing the silver- impregnated collagen cuff with the bedside tunneled subclavian catheter. JPEN J Parenter Enteral Nutr. 1993;17:61–63.
Barrett N, Spencer S, McIvor J, Brown EA. Subclavian stenosis: a major complication of subclavian dialysis catheters. Nephrol Dial Transplant. 1988;3(4):423–425. [PubMed: 3140128].
Cimochowski GE, Worley E, Rutherford WE, et al. Superiority of the internal jugular over the subclavian access for temporary dialysis. Nephron 1990;54:154–161.
Cimochowski GE, Worley E, Rutherford WE, Sartain J, Blondin J, Harter H. Superiority of the internal jugular over the subclavian access for temporary dialysis. Nephron. 1990;54(2):154–161. [PubMed: 2314526].
Edward G. Clark Jeffrey H. Barsuk. Temporary hemodialysis catheters: recent advances Kidney International (2014) 86,888–895. Doi:10.1038/ki.2014.162.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012;120:179–184.
Konner K. Subclavian haemodialysis access: is it still justified in 1995? Nephrology Dialysis Transplantation. 1995;10:1988–1991.
Marik PE, Flemmer M, HarrisonW. The risk of catheter-related bloodstream infection with femoral venous catheters as compared to subclavian and internal jugular venous catheters: a systematic review of the literature and meta-analysis. Crit Care Med 2012;40(8):2479–2485.
Merrer J, De JB, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. Jama. 2001;286(6):700–707. [PubMed: 11495620].
Nagashima G, Kikuchi T, Tsuyuzaki H, et al. To reduce catheter-related bloodstream infections: is the subclavian route better than the jugular route for central venous catheterization? J Infect Chemother. 2006; 12(6):363–365. [PubMed: 17235641].
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: vascular access. Am J Kidney Dis 2006;48:S176–S307.
O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
Parienti JJ, du Cheyron D, Timsit JF, et al. Meta-analysis of subclavian insertion and nontunneled central venous catheter–associated infection risk reduction in critically ill adults. Crit Care Med 2012;40(5):1627–1634.
Ruesch S, Walder B, Tramer MR. Complications of central venous catheters: internal jugular versus subclavian access – a systematic review. Crit Care Med. 2002; 30(2):454–460. [PubMed: 11889329].
Sadoyama G, Gontijo FPP. Comparison between the jugular and subclavian vein as insertion site for central venous catheters: microbiological aspects and risk factors for colonization and infection. Braz J Infect Dis. 2003;7(2):142–148. [PubMed: 12959686].
Sands J. Vascular access: the past present and future. Blood Purif 2009 27:22–27;4.
Schillinger F, Schillinger D, Montagnac R, Milcent T. Post catheterisation vein stenosis in haemodialysis: comparative angiographic study of 50 subclavian and 50 internal jugular accesses. Nephrol Dial Transplant. 1991;6(10):722–724. [PubMed: 1754109] 91.
Trottier SJ, Veremakis C, O'Brien J, Auer AI. Femoral deep vein thrombosis associated with central venous catheterization: results from a prospective, randomized trial. Crit Care Med. 1995;23(1):52–59. [PubMed: 8001386].
Vasquez MA. Vascular access for dialysis: recent lessons and new insights. Curr Nephrol Hypertens 2009;18:116–121.
1.9. Мы рекомендуем всем избегать использования бедренной локализации для нетуннелированного катетера для гемодиализа взрослым пациентам при состояниях при ХБП-5.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Нарушения функционирования и укорочение актуариальной выживаемости доступа чаще наблюдались при локализации катетеров для гемодиализа в бедренных венах по сравнению с яремными. При этом констатировалось более частое нарушение функции катетера, установленного в бедренную вену по сравнению с правой яремной веной, и достоверно более частую дисфункцию катетеров, установленных в левую яремную вену по сравнению с бедренной. Рециркуляция чаще наблюдается при катетеризации бедренных, чем яремных или подключичных вен, особенно при использовании коротких бедренных катетеров для гемодиализа. Не следует устанавливать катетер в бедренную вену во избежание риска развития стеноза подвздошной вены, если планируется анастомоз почечной вены при трансплантации донорской почки. Наличие катетера в бедренной вене, кроме того, ограничивает подвижность больного, особенно при длительном оказании медицинской помщи методами диализа.
Dugue AE, Levesque SP, Fischer MO et al. Vascular access sites for acute renal replacement in intensive care units. Clin J Am Soc Nephrol 2012;7:70–77.
Ge X, Cavallazzi R, Li C et al. Central venous access sites for the prevention of venous thrombosis, stenosis and infection. Cochrane Database of Systematic Reviews. 2012: Art.No.:CD004084. Doi: 10.1002/14651858.CD004048.pub3.
Goetz AM, Wagener MM, Miller JM, Muder RR. Risk of infection due to central venous catheters: effect of site of placement and catheter type. Infect Control Hosp Epidemiol. 1998;19(11):842– 845. [PubMed: 9831940].
Hryszko T, Brzosko S, Mazerska M, et al. Risk factors of nontunneled noncuffed hemodialysis catheter malfunction. A prospective study. Nephron Clin Pract 2004; 96:43–47.
Klouche K, Amigues L, Deleuze S, Beraud JJ, Canaud B Complications, effects on dialysis dose, and survival of tunneled femoral dialysis catheters in acute renal failure. Am J Kidney. Dis. 2007 Jan;49(1):99–108.
Leblanc M, Fedak S, Mokris G, et al. Blood recirculation in temporary central catheters for acute hemodialysis. Clin Nephrol 1996;45:315–319.
Lemaire X, Morena M, Leray-Moragués H et al. Analysis of risk factors for catheter-related bacteremia in 2000 permanent dual catheters for hemodialysis. Blood Purif. 2009;28:21–28.
Liangos O, Rao M, Ruthazer R, et al. Factors associated with urea reduction ratio in acute renal failure. Artif Organs 2004;28:1076–1081.
Little MA, Conlon PJ, Walshe JJ. Access recirculation in temporary hemodialysis catheters as measured by the saline dilution technique. Am J Kidney. Dis 2000;36:1135–1139.
Lorente L, Henry C, Martin MM, Jimenez A, Mora ML. Central venous catheter-related infection in a prospective and observational study of 2,595 catheters. Crit Care. 2005;9(6):R631–R635. [PubMed: 16280064].
Marik PE, Flemmer M, HarrisonW. The risk of catheter-related bloodstream infection with femoral venous catheters as compared to subclavian and internal jugular venous catheters: a systematic review of the literature and meta-analysis. Crit Care Med 2012;40(8):2479–2485.
Merrer J, De JB, Golliot F, et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. Jama. 2001; 286(6):700–707. [PubMed: 11495620].
Mohamed H, Ali A, Browne LD, O'Connell NH, Casserly L, Stack AG, Hussein WF Determinants and outcoms of access-related blood-stream infections among Irish haemodialysis patients; a cohort study. BMC Nephrol. 2019. Feb 26;20(1):68. Doi: 10.1186/s12882-019-1253-x.
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: vascular access. Am J Kidney Dis 2006;48:S176–S307.
Naumovic RT, Jovanovic DB, Djukanovic LJ. Temporary vascular catheters for hemodialysis: a 3-year prospective study. Int J Artif Organs 2004;27:848–854.
Oliver MJ, Callery SM, Thorpe KE et al. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: a prospective study. Kidney Int 2000;58:2543–2545.
Parienti JJ, Megarbane B, Fischer MO, et al. Catheter dysfunction and dialysis performance according to vascular access among 736 critically ill adults requiring renal replacement therapy: a randomized controlled study. Crit Care Med 2010;38:1118–1125.
Parienti JJ, Thirion M, Megarbane B, et al. Femoral vs jugular venous catheterization and risk of nosocomial events in adults requiring acute renal replacement therapy: a randomized controlled trial. Jama. 2008;299(20):2413–2422. [PubMed: 18505951].
Parienti JJ, Thirion M, Megarbane B, et al. Femoral vs jugular venous catheterization and risk of nosocomial events in adults requiring acute renal replacement therapy: a randomized controlled trial. Jama. 2008;299(20):2413–2422. [PubMed: 18505951].
Prabhu MV, Juneja D, Gopal P, et al. Ultrasound-guided femoral dialysis access placement: a single-center randomized trial. Clin J Am Soc Nephrol. 2010;5:235–239.
Pronovost P. Interventions to decrease catheter-related bloodstream infections in the ICU: the Keystone Intensive Care Unit Project. Am J Infect Control 2008;36:S171;e171–175.
2. Условия для введения катетера для диализа
2.1. Рекомендуем: чрезкожное введение туннелированного катетера для гемодиализа и обмен по проводнику для взрослых пациентов должны рассматриваться в качестве хирургической процедуры и производиться обученным опытным персоналом в специальной зоне в асептических условиях.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Установка катетера должна производиться в строгом соответствии с санитарно-эпидемиологическими правилами, в том числе с максимальным использованием барьерных методов. Требование специальных условий для введения туннелированного катетера для гемодиализа может стать препятствием для своевременного начала лечения и может быть небезопасным или неосуществимым, если это требует перевода пациента из интенсивной терапии в другие условия. Когда невозможно обеспечить соблюдение асептических условий (т.е. введение катетеры во время экстренной медицинской помощи), необходимо заменить катетер как можно скорее – в течение 48 часов.
Aboelela SW, Stone PW, Larson EL. Effectiveness of bundled behavioural interventions to control healthcare-associated infections: a systematic review of the literature. J Hosp Infect 2007;66(2):101–108.
Blot K, Bergs J, Vogelaers D, et al. Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect. Dis. 2014;59:96–105. Doi: 10.1093/cid/ciu239.
Bonawitz SC, Hammell EJ, Kirkpatrick JR. Prevention of central venous catheter sepsis: A prospective randomized trial. Am Surg. 1991;57:618–623.
Brunelli SM, Van Wyck DB, Njord L, Ziebol RJ, Lynch LE, Killion DP. Cluster-randomized trial of devices to prevent catheter-related bloodstream infection. J Am Soc Nephrol: JASN. 2018;29(4):1336–1343.
Burrell AR, McLaws M-L, Murgo M et al. Aseptic insertion of central venous lines to reduce bacteraemia. Medical Journal of Australia. 2011;194:583–587.
Capdevila JA, Segarra A, Pahissa A. Catheter-related bacteremia in patients undergoing hemodialysis. Ann Intern Med. 1998;128(7):600. [PubMed: 9518412].
Coopersmith CM, Rebmann TL, Zack JE, et al. Effect of an education program on decreasing catheter-related bloodstream infections in the surgical intensive care unit. Crit Care Med. 2002;30(1):59–64. [PubMed: 11902288].
Coopersmith CM, Zack JE, Ward MR, et al. The impact of bedside behavior on catheter-related bacteremia in the intensive care unit. Arch Surg. 2004; 139(2):131–136. [PubMed: 14769568].
Davis D, O'Brien MA, Freemantle N, Wolf FM, Mazmanian P, Taylor-Vaisey A. Impact of formal continuing medical education: do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes? Jama. 1999; 282(9):867– 874. [PubMed: 10478694].
Eggimann P, Harbarth S, Constantin MN, Touveneau S, Chevrolet JC, Pittet D. Impact of a prevention strategy targeted at vascular-access care on incidence of infections acquired in intensive care. Lancet. 2000;355(9218):1864–1868. [PubMed: 10866442].
Fluk R and Kumwenda MJ, Prevention of catheter related infections. Guideline 5.1, in Vascular access for haemodialysis. 2011, UK Renal Association.
Funaki B, Zaleski GX, Leef JA et al. Radiologic placement of tunneled hemodialysis catheters in occluded neck, chest, or small thyrocervical collateral veins in central venous occlusion. Radiology. 2001;218:471–476.
George A, Tokars JI, Clutterbuck EJ et al. Reducing dialysis associated bacteraemia, and recommendations for surveillance in the United Kingdom: prospective study. BMJ 2006;332:1435.
Hawes ML. A proactive approach to combating venous depletion in the hospital setting. J Infus Nurs. 2007;30(1):33–44. [PubMed: 17228197].
Huang EY, Chen C, Abdullah F, et al. Strategies for the prevention of central venous catheter infections: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee systematic review. J Pediatr Surg 2011;46(10):2000–2011.
Hymes JL, Mooney A, Van Zandt C, Lynch L, Ziebol R, Killion D. Dialysis Catheter-Related Bloodstream Infections: A Cluster-Randomized Trial of the ClearGuard HD Antimicrobial Barrier Cap. Am J Kidney Dis. 2017;69(2):220–227.
Ma IW, Brindle ME, Ronksley PE, Lorenzetti DL, Sauve RS, Ghali WA. Use of simulation-based education to improve outcomes of central venous catheterization: a systematic review and meta-analysis. Acad Med 2011;86(9):1137–1147.
Marschall J, Mermel LA, Classen D, et al. Strategies to prevent central lineassociated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol 2008;29 (Suppl 1):S22–30.
Marschall J, Mermel LA, Fakih M. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(7):753–771.
McCann M, Moore ZE. Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database Systematic Review 2010;20(1):CD00689.
Mermel LA, Maki DG. Infectious complications of Swan-Ganz pulmonary artery catheters. Pathogenesis, epidemiology, prevention, and management. Am J Respir Crit Care Med. 1994;149(4 Pt 1):1020–1036. [PubMed: 8143037]. 127.
Mermel LA, McCormick RD, Springman SR, Maki DG. The pathogenesis and epidemiology of catheter-related infection with pulmonary artery Swan-Ganz catheters: a prospective study utilizing molecular subtyping. Am J Med. 1991; 91:197S–205S. [PubMed: 1928165].
Nehme AE. Nutritional support of the hospitalized patient. The team concept. Jama. 1980;243(19):1906–1908. [PubMed: 6767864].
O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
Patel PR, Kallen AJ, Arduino MJ: Epidemiology, surveillance, and prevention of bloodstream infections in hemodialysis patients. Am J Kidney Dis 56:566–577, 2010.
Pierce CA, Baker JJ. A nursing process model: quantifying infusion therapy resource consumption. J Infus Nurs. 2004;27(4):232–244. [PubMed: 15273630].
Powell S, Chan TY, Bhat R et al. A retrospective comparative study of tunneled haemodialysis catheters inserted through occluded or collateral veins versus conventional methods. Cardiovascular & Interventional Radiology. 2010;33:744–750.
Pratt RJ, Pellowe CM, Wilson JA, et al. epic2: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect, 2007;65(Suppl 1):S1–64.
Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, Sexton B, Hyzy R, Welsh R, Roth G, Bander J, Kepros J, Goeschel C. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725–2732.
Pronovost PJ, Goeschel CA, Colantuoni E et al. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study. BMJ, 2010;340:309.
Raad II, Hohn DC, Gilbreath BJ et al Prevention of central venous catheter-related infections by using maximal sterile barrier precautions during insertion. Infect Control Hosp Epidemiol 1994;15:231–238 (B).
Raad II, Luna M, Khalil SA, Costerton JW, Lam C, Bodey GP. The relationship between the thrombotic and infectious complications of central venous catheters. Jama. 1994;271(13):1014– 1016. [PubMed: 8139059].
Ranasinghe JS, Lee AJ, Birnbach DJ. Infection associated with central venous or epidural catheters: how to reduce it? Curr Opin Anaesthesiol. 2008 Jun;21(3):386–390. Doi: 10.1097/ACO.0b013e3282fd68d5. Review.
Rosenblum A, Wang W, Ball LK, Latham C, Maddux FW, Lacson E, Jr. Hemodialysis catheter care strategies: a cluster-randomized quality improvement initiative. Am J Kidney Dis. 2014;63(2):259–267.
Safdar N, Abad C. Educational interventions for prevention of healthcare-associated infection: a systematic review. Crit Care Med 2008;36(3):933–940.
Sherertz RJ, Ely EW, Westbrook DM, et al. Education of physicians-in-training can decrease the risk for vascular catheter infection. Ann Intern Med. 2000;132(8):641–648. [PubMed: 10766683].
Silva TN, de Marchi D, Mendes ML et al. Approach to prophylactic measures for central venous catheter-related infections in hemodialysis: a critical review. Hemodial Int 2014;18:15–23.
Tomford JW, Hershey CO. The i.v therapy team: impact on patient care and costs of hospitalization. NITA. 1985;8(5):387–389. [PubMed: 3850385].
Vanholder R, Canaud B Fluck R et al. Diagnosis, prevention and treatment of haemodialysis catheter-related bloodstream infections (CRBSI): a position statement of European Renal Best Practice (ERBP). NDT Plus 2010;3:234–246. Doi: 10.1093/ndtplus/sfq041.
Weaver SJ, Lubomksi LH, Wilson RF, Pfoh ER, Martinez KA, Dy SM. Promoting a culture of safety as a patient safety strategy: a systematic review. Ann Intern Med 2013;158(5 pt 2):369– 374.
Wivell W, Bettmann MA, Baxter B. Outcomes and performance of the Tesio twin catheter system placed for hemodialysis access. Radiology 2001;221:697–703.
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
2.2. Hекомендуем медицинским работникам при чрезкожном введении и обмене по проводнику катетера для гемодиализа выполнять максимально барьерные меры предосторожности, включая медицинские шапочки, защитные очки, маски, стерильный халат, стерильные перчатки и стерильную простыню для всего тела с отверстием для операционного поля.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Allon M, Depner TA, Radeva M, Bailey J, Beddhu S, Butterly D, Coyne DW, Gassman JJ, Kaufman AM, Kaysen GA, Lewis JA, Schwab SJ; HEMO Study Group: Impact of dialysis dose and membrane on infection-related hospitalization and death: Results of the HEMO Study. J AmSoc Nephrol 14:1863–1870, 2003.
Aslam S, Vaida F, Ritter M, Mehta RL. Systematic review and metaanalysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol: JASN. 2014;25(12):2927–2941.
Blot K, Bergs J, Vogelaers D, et al. Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect Dis. 2014;59:96–105. Doi: 10.1093/cid/ciu239.
Carrer S, Bocchi A, Bortolotti M, et al. Effect of different sterile barrier precautions and central venous catheter dressing on the skin colonization around the insertion site. Minerva Anestesiol. 2005;71(5):197–206. [PubMed: 15834348].
Hymes JL, Mooney A, Van Zandt C, Lynch L, Ziebol R, Killion D. Dialysis Catheter-Related Bloodstream Infections: A Cluster-Randomized Trial of the ClearGuard HD Antimicrobial Barrier Cap. Am J Kidney Dis. 2017;69(2):220–227.
Lemaire X, Morena M, Leray-Moragues H et al. Analysis of risk factors for catheter-related bacteremia in 2000 permanent dual catheters for hemodialysis. Blood Purif 2009;28:21–28.
Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clinic proceedings Mayo Clinic. 2006;81(9):1159–1171. [PubMed: 16970212].
McCann M, Moore ZE. Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database Systematic Review 2010;20(1):CD00689.
McLure HA, Talboys CA, Yentis SM, Azadian BS. Surgical face masks and downward dispersal of bacteria. Anaesthesia. 1998 Jul;53(7):624–626.
Mermel LA, Maki DG. Infectious complications of Swan-Ganz pulmonary artery catheters. Pathogenesis, epidemiology, prevention, and management. Am J Respir Crit Care Med. 1994;149(4 Pt 1):1020–1036. [PubMed: 8143037].
Quittnat Pelletier F, Joarder M, Poutanen SM, Lok CE. Evaluating approaches for the diagnosis of hemodialysis catheter-related bloodstream infections. Clin J Am Soc Nephrol: CJASN. 2016;11(5):847–854.
Raad II, Hohn DC, Gilbreath BJ, et al. Prevention of central venous catheter-related infections by using maximal sterile barrier precautions during insertion. Infect Control Hosp Epidemiol. 1994; 15:231–238. [PubMed: 8207189].
Ranucci M, Isgro G, Giomarelli PP, et al. Impact of oligon central venous catheters on catheter colonization and catheter-related bloodstream infection. Crit Care Med. 2003; 31(1):52–59. [PubMed: 12544993].
Rosenblum A, Wang W, Ball LK, Latham C, Maddux FW, Lacson E, Jr. Hemodialysis catheter care strategies: a cluster-randomized quality improvement initiative. Am J Kidney Dis. 2014;63(2):259–267.
Sherertz RJ, Ely EW, Westbrook DM, et al. Education of physicians-in-training can decrease the risk for vascular catheter infection. Ann Intern Med. 2000;132(8):641–648. [PubMed: 10766683].
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004; 39(3):309–317. [PubMed: 15306996].
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10 июня 2016 года)
2.3. Рекомендуем периодически оценивать знания и соблюдение строгих санитарно-гигиенических мер всем персоналом, принимающим участие в катетеризации и уходе за катетером для гемодиализа и проводящим другие манипуляции с ним.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Необходимо проводить переподготовку и систематическое обучение медицинского персонала руководящим принципам инфекционного контроля и для предотвращения инфекций, связанных с катетером для диализа, правилам работы, надлежащей техники, постановке и уходу за сосудистым катетером, показаниям для предписания катетера в качестве доступа для диализа. Необходимо признать необходимость междисциплинарного подхода к обеспечению идеального ухода за сосудистым доступом.
Aboelela SW, Stone PW, Larson EL. Effectiveness of bundled behavioural interventions to control healthcare-associated infections: a systematic review of the literature. J Hosp Infect 2007; 66(2):101–108.
Blot K, Bergs J, Vogelaers D, et al. Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect Dis. 2014;59:96–105. Doi:10.1093/cid/ciu239.
Bonawitz SC, Hammell EJ, Kirkpatrick JR. Prevention of central venous catheter sepsis: A prospective randomized trial. Am Surg. 1991;57:618–623.
Brunelli SM, Van Wyck DB, Njord L, Ziebol RJ, Lynch LE, Killion DP. Cluster-randomized trial of devices to prevent catheter-related bloodstream infection. J Am Soc Nephrol: JASN. 2018;29(4):1336–1343.
Coopersmith CM, Rebmann TL, Zack JE, et al. Effect of an education program on decreasing catheter-related bloodstream infections in the surgical intensive care unit. Crit Care Med. 2002;30(1):59–64. [PubMed: 11902288].
Coopersmith CM, Zack JE, Ward MR, et al. The impact of bedside behavior on catheter-related bacteremia in the intensive care unit. Arch Surg. 2004;139(2):131–136. [PubMed: 14769568].
Eggimann P, Harbarth S, Constantin MN, Touveneau S, Chevrolet JC, Pittet D. Impact of a prevention strategy targeted at vascular-access care on incidence of infections acquired in intensive care. Lancet. 2000;355(9218):1864–1868. [PubMed: 10866442].
Higuera F, Rosenthal VD, Duarte P, Ruiz J, Franco G, Safdar N. The effect of process control on the incidence of central venous catheter-associated bloodstream infections and mortality in intensive care units in Mexico. Crit Care Med. 2005;33(9):2022–2027. [PubMed: 16148475].
Jingjing Zhang, Renee A. Burr, Heena S. Sheth, Beth Piraino Organism-specific bacteremia by hemodialysis access Clinical Nephrology. Vol. 86. No. 3. 2016 (141–146).
Ma IW, Brindle ME, Ronksley PE, Lorenzetti DL, Sauve RS, Ghali WA. Use of simulation-based education to improve outcomes of central venous catheterization: a systematic review and meta-analysis. Acad Med 2011;86(9):1137–1147.
McCann M, Moore ZE. Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database Systematic Review 2010;20(1):CD00689.
Palomar M, Álvarez-Lerma F, Riera A, et al. Impact of a national multimodal intervention to prevent catheter-related bloodstream infection in the ICU: the Spanish experience. Crit Care Med. 2013;41:2364–2372. Doi:10.1097/CCM. 0b013e3182923622.
Pronovost P. Interventions to decrease catheter-related bloodstream infections in the ICU. The Keystone Intensive Care Unit Project. Am J Infect Control 2008;36:S171; e171–175.
Rosenblum A, Wang W, Ball LK, Latham C, Maddux FW, Lacson E, Jr. Hemodialysis catheter care strategies: a cluster-randomized quality improvement initiative. Am J Kidney Dis. 2014;63(2):259–267.
Safdar N, Abad C. Educational interventions for prevention of healthcare-associated infection: a systematic review. Crit Care Med 2008;36(3):933–940.
Sherertz RJ, Ely EW, Westbrook DM, et al. Education of physicians-in-training can decrease the risk for vascular catheter infection. Ann Intern Med. 2000;132(8):641–648. [PubMed: 10766683].
Warren DK, Cosgrove SE, Diekema DJ, et al. A multicenter intervention to prevent catheterassociated bloodstream infections. Infect Control Hosp Epidemiol. 2006;27(7):662–669. [PubMed: 16807839].
Warren DK, Zack JE, Cox MJ, Cohen MM, Fraser VJ. An educational intervention to prevent catheter-associated bloodstream infections in a nonteaching, community medical center. Crit Care Med. 2003;31(7):1959–1963. [PubMed: 12847389].
Warren DK, Zack JE, Mayfield JL, et al. The effect of an education program on the incidence of central venous catheter-associated bloodstream infection in a medical ICU. Chest. 2004;126(5):1612–1618. [PubMed: 15539735].
Yoo S, Ha M, Choi D, Pai H. Effectiveness of surveillance of central catheter-related bloodstream infection in an ICU in Korea. Infect Control Hosp Epidemiol. 2001; 22(7):433–436. [PubMed: 11583212].
2.4. Предлагаем принимать решение о внедрении в практику новых технологий или расходных материалов, связанных с использованием катетера для гемодиализа, на основании данных анализа заболеваемости инфекций кровотока.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Комментарии. Изменение знаний, технологий контроля инфекции должно приводить к изменению предупредительных мер инфицирования. Необходимо учитывать баланс между эффективностью, стоимостью и возможностью медицинской помощи медицинской организации. Эффективность внедрения в работу современных материалов и технологий ухода за катетером для профилактики эндогенного инфицирования катетера и места выхода катетера следует оценивать в клинической практике, наблюдая за частотой, динамикой и этиологической структурой заболеваемости КАИК.
Lok CE and Mokrzycki MH. Prevention and management of catheter-related infection in hemodialysis patients. Kidney international. 2011.
Marschall J, Mermel LA, Classen D, et al. Strategies to prevent central lineassociated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol 2008;29(Suppl 1):S22–30.
Mermel LA, Farr BM, Sherertz RJ et al. Infectious Diseases Society of America; American College of Critical Care Medicine; Society for Healthcare Epidemiology of America. Guidelines for the management of intravascular catheter-related infections. Clin Infect Dis 2001;32:1249–1272.
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: vascular access. Am J Kidney Dis 2006;48:S176–S307.
O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
Pratt RJ, Pellowe CM, Wilson JA, et al: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 2007;65(Suppl 1):S1–64.
Rosenblum A, Wang W, Ball LK, Latham C, Maddux FW, Lacson E Jr.Hemodialysis catheter care strategies: a cluster-randomized quality improvement initiative. Am J Kidney Dis. 2014. Feb;63(2):259–267. Doi: 10.1053/j.ajkd.2013.08.019. Epub 2013 Dec 2.
Tordoir J, Canaud B, Haage P et al. EBPG on Vascular Access. Nephrology Dialysis Transplantation. 2007;22:ii88–117.
USRDS: US Renal Data System. Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. 2009. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD.
Vanholder R, Canaud B Fluck R et al. Diagnosis, prevention and treatment of haemodialysis catheter-related bloodstream infections (CRBSI): a position statement of European Renal Best Practice (ERBP). NDT Plus 2010;3:234–246. Doi:10.1093/ndtplus/sfq041.
2.5. Рекомендуем учет всех случаев инфекций кровотока, связанных с катетером для гемодиализа, по дате заболевания, основанной на стандартном определении случая.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. Постоянное эпидемиологическое наблюдение за всеми, кто использует сосудистый доступ ЦВК для диализа, наиболее информативно, однако его проведение связано с большими трудозатратами.
Centers for M, Medicaid Services HHS. Medicare Program; endstage renal disease prospective Payment system, Payment for renal dialysis Services Furnished to Individuals with Acute kidney Injury, and end-stage renal disease Quality Incentive Program. Final rule. Fed Regist. 2017;82(210):50738–50797.
Lai CF, Liao CH, Pai MF, et al. Nasal carriage of methicillin-resistant Staphylococcus aureus is associated with higher all-cause mortality in hemodialysis patients. Clin J Am Soc Nephrol: CJASN. 2011;6(1):167–174.
Patel PR, Kallen AJ. Bloodstream infection prevention in ESRD: forging a pathway for success. Am J Kidney Dis. 2014 Feb;63(2):180–182. Doi: 10.1053/j.ajkd.2013.11.003.
Patel PR, Yi SH, Booth S, Bren V, Downham G, Hess S, Kelley K, Lincoln M, Morrissette K, Lindberg C, Jernigan JA, Kallen AJ. Bloodstream infection rates in outpatient hemodialysis facilities participating in a collaborative prevention effort: a quality improvement report. Am J Kidney Dis. 2013 Aug;62(2):322–330. Doi: 10.1053/j.ajkd.2013.03.011. Epub 2013 May 13.
Pop-Vicas A, Strom J, Stanley K, D’Agata EM. Multidrug-resistant gram-negative bacteria among patients who require chronic hemodialysis. Clin J Am Soc Nephrol: CJASN. 2008;3(3):752–758.
Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, Sexton B, Hyzy R, Welsh R, Roth G, Bander J, Kepros J, Goeschel C. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006 Dec 28;355(26):2725–2732.
Taylor GD, McKenzie M, Buchanan-Chell M, Caballo L, Chui L, Kowalewska-Grochowska K. Central venous catheters as a source of hemodialysis-related bacteremia. Infect Control Hosp Epidemiol. 1998;19(9):643–646.
Tordoir J, Canaud B, Haage P et al. EBPG on Vascular Access. Nephrology Dialysis Transplantation. 2007;22:ii88–117.
Vanholder R, Canaud B Fluck R et al. Diagnosis, prevention and treatment of haemodialysis catheter-related bloodstream infections (CRBSI): a position statement of European Renal Best Practice (ERBP). NDT Plus 2010;3:234–246. Doi: 10.1093/ndtplus/sfq041.
Vassalotti JA, Jennings WC, Beathard GA, et al. Fistula First Breakthrough Initiative: targeting catheter last in fistula first. Semin Dial. 2012;25:303– 310.
3. Контроль введения катетера для диализа
3.1. Рекомендуем проводить чрезкожную катетеризацию под обязательным ультразвуковым контролем, при любом типе и локализации центрального венозного катетера на взрослых пациентах сразу после введения катетера и перед первым его использованием, при локализации катетера для диализа во внутренней яремной или подключичной вене, дополнительно проводится диагностическая рентгенография органов грудной клетки.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Для контроля расположения дистального сегмента катетера перед использованием и своевременной диагностики механических повреждений при катетеризации следует выполнять рентген-контроль органов грудной клетки после введения ЦВК в вены брахеоцефального ствола.
Allon M, Brouwer-Maier DJ, Abreo K, Baskin KM, Bregel K, Chand DH, Easom AM, Mermel L, Mokrzycki MH, Patel PR, Roy-ChaudhuryP, ShenoyS, Valentini RP, Wasse H Recommended Clinical Trial End Points for Dialysis Catheters. Clin J Am Soc Nephrol. 2018 Mar 7;13(3):495–500. Doi: 10.2215/CJN.12011116. Epub 2017 Jul 20.
Bansal R, Agarwal S, Tiwari SC, Dash SC. A prospective randomized study to compare ultrasound-guided with non-ultrasound guided double lumen internal jugular catheter insertion as a temporary hemodialysis access. Ren Fail. 2005;27:561–564.
Clark EG, Schachter ME, Palumbo A et al. Temporary hemodialysis catheter placement by nephrology fellows: implications for nephrology training. Am J Kidney Dis 2013;62:474–480.
Farrell J, Gellens M. Ultrasound-guided cannulation versus the landmarkguided technique for acute haemodialysis access. Nephrol Dial Transplant 1997;12:1234–1237.
Gallieni M. Central vein catheterization of dialysis patients with real time ultrasound guidance. J Vasc Access 2000;1:10–14.
Hind D, Calvert N, McWilliams R, et al. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ? 2003;327:361.
Hsu JH, Wang CK, Chu KS, et al. Comparison of radiographic landmarks and the echocardiographic SVC/RA junction in the positioning of longterm central venous catheters. Acta Anaesthesiol Scand 2006;50:731–735.
Hull JE, Jennings WC, Cooper RI, et al. The pivotal multicenter trial of ultrasound-guided percutaneous arteriovenous fistula creation for hemodialysis access. J Vasc Interv Radiol. 2018;29:149–158.
Karakitsos D, Labropoulos N, De Groot E, et al. Real-time ultrasound-guided catheterisation of the internal jugular vein: a prospective comparison with the landmark technique in critical care patients. Crit Care 2006;10:R162.
Koroglu M, Demir M, Koroglu B et al. Percutaneous placement of central venous catheters: comparing the anatomical landmark method with the radiologically guided technique for central venous catheterization through the internal jugular vein in emergent hemodialysis patients. Acta Radiologica. 2006;47:43–47.
Kusminsky RE. Complications of central venous catheterization. J Am Coll Surg 2007;204:681–696.
Kwon TH, Kim YL, Cho DK. Ultrasound-guided cannulation of the femoral vein for acute haemodialysis access. Nephrol Dial Transplant 1997;12:1009–1012.
Leung J, Duffy M, Finckh A. Real-time ultrasonographically-guided internal jugular vein catheterization in the emergency department increases success rates and reduces complications: a randomized, prospective study. Ann Emerg Med 2006;48:540–547.
Lin BS, Huang TP, Tang GJ, Tarng DC, Kong CW. Ultrasoundguided cannulation of the internal jugular vein for dialysis vascular access in uremic patients. Nephron. 1998;78:423–428.
McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med 2003;348 1123–1133.
Motta ER, da Silva MSC, Abensur H et al. Insertion of tunneled hemodialysis catheters without fluoroscopy. The journal of vascular access. 2010;11:138.
Nadig C, Leidig M, Schmiedeke T, Hoffken B. The use of ultra- € sound for the placement of dialysis catheters. Nephrol Dial Transplant. 1998;13:978–981.
National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: vascular access. Am J Kidney Dis 2006;48:S176–S307.
Prabhu MV, Juneja D, Gopal P, et al. Ultrasound-guided femoral dialysis access placement: a single-center randomized trial. Clin J Am Soc Nephrol. 2010;5:235–239.
Puel V, Caudry M, Le Metayer P, et al. Superior vena cava thrombosis related to catheter malposition in cancer chemotherapy given through implanted ports. Cancer 1993;72:2248–2252.
Rabindranath KS, Kumar E, Shail R, Vaux E. Use of real-time ultrasound guidance for the placement of hemodialysis catheters: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis. 2011;58:964–970.
Randolph AJ, Cook DJ, Gonzales CA, Pribble CG. Ultrasound guidance for placement of central venous catheters: a meta-analysis of the literature. Crit Care Med. 1996;24:2053–2058.
Schummer W, Sakr Y, Schummer C. Towards optimal central venous catheter tip position. In: Vincent J-L (ed). Intensive Care Medicine. Springer Verlag: Berlin, Germany, 2008.581–590.
Sirvent AE, Enriquez R, Millan I et al. Severe hemorrhage because of delayed iliac vein rupture after dialysis catheter placement: is it preventable? Hemodial Int 2012;16:315–319.
Vesely TM. Central venous catheter tip position: a continuing controversy. J Vasc Interv Radiol 2003;14:527–534.
Yevzlin AS, Song GU, Sanchez RJ et al. Fluoroscopically guided vs modified traditional placement of tunneled hemodialysis catheters: clinical outcomes and cost analysis. Journal of Vascular Access. 2007;8:245–51.
Zollo A, Cavatorta F, Galli S. Ultrasound-guided cannulation of the femoral vein for acute hemodialysis access with silicone catheters. J Vasc Access 2001;2:56–59.
4. Манипуляции при введении катетера для диализа
4.1. Мы полагаем, что волосы в области локализации любого типа центрального венозного катетера следует удалzть непосредственно перед его введением, используя медицинские стригущие машинки.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Комментарии. Пациенты должны придерживаться правил личной гигиены. Бритье волос бритвой не рекомендовано, поскольку приводит к повреждению кожи и более частому инфицированию раны входного отверстия катетера.
CDC Vital Signs. Making health care safer: Reducing bloodstream infections. 2011. https://www.cdc.gov/vitalsigns/ pdf/2011-03-vitalsigns.pdf. Accessed October 4, 2018.
Centers for Disease C, Prevention. Reducing bloodstream infections in an outpatient hemodialysis center–New Jersey, 2008-2011. MMWR Morbidity Mortality Weekly Rep. 2012;61(10):169–173.
George A, Tokars JI, Clutterbuck EJ et al. Reducing dialysis associated bacteraemia, and recommendations for surveillance in the United Kingdom: prospective study. BMJ, 2006;332:1435.
Huang EY, Chen C, Abdullah F, et al. Strategies for the prevention of central venous catheter infections: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee systematic review. J Pediatr Surg 2011;46(10):2000–2011.
Kaplowitz LG, Comstock JA, Landwehr DM, Dalton HP, Mayhall CG. A prospective study of infections in hemodialysis patients: patient hygiene and other risk factors for infection. Infect Control Hosp Epidemiol 1988;9:534–541.
Patel PR, Kallen AJ, Arduino MJ: Epidemiology, surveillance, and prevention of bloodstream infections in hemodialysis patients. Am J Kidney Dis 56:566–577, 2010.
Palomar M, Álvarez-Lerma F, Riera A, et al. Impact of a national multimodal intervention to prevent catheter-related bloodstream infection in the ICU: the Spanish experience. Crit Care Med. 2013;41:2364–2372. Doi:10.1097/CCM. 0b013e3182923622.
Pronovost PJ, Goeschel CA, Colantuoni E et al. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study. BMJ, 2010;340:309.
Taylor G, Gravel D, Johnston L, Embil J, Holton D, Paton S. Prospective surveillance for primary bloodstream infections occurring in Canadian hemodialysis units. Infect Control Hosp Epidemiol. 2002;23(12):716–720.
Tokars JI, Miller ER, Stein G: New national surveillance system for hemodialysis-associated infections: Initial results. Am J Infect Control 30:288–295, 2002.
4.2. Рекомендуем медицинскому персоналу проводить хирургическую обработку рук при введении и обмене по проводнику при любом типе и локализации центрального венозного катетера для гемодиализа взрослых пациентов.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Комментарии. Необходимый уровень деконтаминации рук может быть достигнут только при соблюдении базовых условий гигиены рук.
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
Приказ № 199-ст Росстандарта от 31.03.2015 утвержден ГОСТом Р 52623.3-2015 «Технологии выполнения простых медицинских услуг. Манипуляции сестринского ухода».
4.3. Рекомендуем медицинскому персоналу использовать антисептики для обработки рук при введении и обмене по проводнику катетера для гемодиализа только на спиртовой основе, которая для достижения оптимальной антимикробной активности должна иметь в составе от 75 до 80% объемного содержания этанола, изопропанола, н-пропанола или их сочетание.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Время обработки рук спиртосодержащим антисептиком определено в инструкции производителя.
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06. 2016).
O'Grady NP, Alexander M, Burns LA et al. Healthcare Infection Control Practices Advisory Committee (HICPAC): Guidelines for the prevention of intravascular catheter-related infections. Clinical infectious diseases. 2011;52:e162–183.
Jindal K, Chan CT, Deziel C et al. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. Journal of the American Society of Nephrology: JASN. 2006;17:S1.
Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991;338:339–343. [PubMed: 1677698].
Mimoz O, Lucet JC, Kerforne T, Pascal J, Souweine B, Goudet V, Mercat A, Bouadma L, Lasocki S, Alfandari S, Friggeri A, Wallet F, Allou N, Ruckly S, Balayn D, Lepape A, Timsit JF; CLEAN trial investigators. Skin antisepsis with chlorhexidine-alcohol versus povidone iodine-alcohol, with and without skin scrubbing, for prevention of intravascular-catheter-related infection (CLEAN): an open-label, multicentre, randomised, controlled, two-by-two factorial trial. Lancet. 2015 Nov 21;386(10008):2069–2077. Doi: 10.1016/S0140-6736(15)00244-5. Epub 2015 Sep 18.
O’Horo JC, Silva GL, Munoz-Price LS, Safdar N. The efficacy of daily bathing with chlorhexidine for reducing healthcare associated bloodstream infections: a meta analysis. Infect Control Hosp Epidemiol 2012;33(3):257–267.
4.4. Рекомендуем для обработки кожных покровов использовать спиртосодержащие препараты на основе гуанидинов (хлоргексидин биглюконат) в концентрации более 1%.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Применение антисептиков не должно заменять гигиенические стандарты. При наличии противопоказаний к применению хлоргексидина (повышенная чувствительность кожи или аллергия) используют 10%-ный водный раствор повидон-йода или 70%-ный спирт могут быть использованы в качестве альтернативы.
Chaiyakunapruk N, Veenstra DL, Lipsky BA et al. Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: a meta-analysis. Ann Intern Med 2002;136:792–801.
Darouiche RO, Wall Jr MJ, Itani KM et al. Chlorhexidine-alcohol versus povidone-iodine for surgical-site antisepsis. N Engl J Med 2010;362:18–26.
Harwood L, Wilson B, Thompson B et al. Predictors of hemodialysis central venous catheter exit-site infections. Cannt Journal. 2008;18:26–35.
Ishizuka M, Nagata H, Takagi K et al. Comparison of 0.05% chlorhexidine and 10% povidone-iodine as cutaneous disinfectant for prevention of central venous catheter-related bloodstream infection: a comparative study. Eur Surg Res 2009;43:286–290.
Jindal K, Chan CT, Deziel C et al. Hemodialysis clinical practice guidelines for the Canadian Society of Nephrology. Journal of the American Society of Nephrology. .JASN, 2006;17:S1.
Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991;338:339–343. [PubMed: 1677698].
Mimoz O, Lucet JC, Kerforne T, Pascal J, Souweine B, Goudet V, Mercat A, Bouadma L, Lasocki S, Alfandari S, Friggeri A, Wallet F, Allou N, Ruckly S, Balayn D, Lepape A, Timsit JF; CLEAN trial investigators. Skin antisepsis with chlorhexidine-alcohol versus povidone iodine-alcohol, with and without skin scrubbing, for prevention of intravascular-catheter-related infection (CLEAN): an open-label, multicentre, randomised, controlled, two-by-two factorial trial. Lancet. 2015. Nov 21;386(10008):2069–2077. Doi: 10.1016/S0140-6736(15)00244-5. Epub 2015 Sep 18.
O’Horo JC, Silva GL, Munoz-Price LS, Safdar N. The efficacy of daily bathing with chlorhexidine for reducing healthcare associated bloodstream infections: a meta analysis. Infect Control Hosp Epidemiol 2012;33(3):257–267.
Paocharoen V, Mingmalairak C, Apisarnthanarak A. Comparison of surgical wound infection after preoperative skin preparation with 4% chlorhexidine [correction of chlohexidine] and povidone iodine: a prospective randomized trial. J Med Assoc Thai 2009;92:898–902.
Parienti JJ, du Cheyron D, Ramakers M, et al. Alcoholic povidone-iodine to prevent central venous catheter colonization: A randomized unit-crossover study. Crit Care Med. 2004;32(3):708–713. [PubMed: 15090951].
Valles J, Fernandez I, Alcaraz D et al. Prospective randomized trial of 3 antiseptic solutions for prevention of catheter colonization in an intensive care unit for adult patients. Infect Control Hosp Epidemiol, 2008;29:847–853.
Maiwald M, Chan ES. The forgotten role of alcohol: a systematic review and meta-analysis of the clinical efficacy and perceived role of chlorhexidine in skin antisepsis. PLoS ONE 2012;7(9):44277.
4.5. Рекомендуем медицинскому персоналу при введении и обмене по проводнику катетера для гемодиализа использовать только стерильные перчатки, которые дополняют гигиеническую обработку рук.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Используют только стерильные перчатки, которые надевают на полностью сухие руки. Используйте новые стерильные перчатки перед работой с новым катетером. Гигиена рук также должна выполняться после снятия перчаток.
Fluk R, Kumwenda MJ, Prevention of catheter related infections. Guideline 5.1, in Vascular access for haemodialysis. 2011, UK Renal Association.
Maiwald M, Chan ES. The forgotten role of alcohol: a systematic review and meta-analysis of the clinical efficacy and perceived role of chlorhexidine in skin antisepsis. PLoS ONE 2012;7(9):e44277.
O’Horo JC, Silva GL, Munoz-Price LS, Safdar N. The efficacy of daily bathing with chlorhexidine for reducing healthcare associated bloodstream infections: a meta analysis. Infect Control Hosp Epidemiol 2012;33(3):257–267.
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
Приказ № 199-ст Росстандарта от 31.03. 2015 утвержден ГОСТом Р 52623.3-2015 «Технологии выполнения простых медицинских услуг. Манипуляции сестринского ухода».
4.6. Предлагаем фиксировать центральный венозный катетер на коже лигатурой или специальным устройством для бесшовной фиксации.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
Приказ № 199-ст Росстандарта от 31.03.2015 утвержден ГОСТом Р 52623.3-2015 «Технологии выполнения простых медицинских услуг. Манипуляции сестринского ухода».
Yamamoto AJ, Solomon JA, Soulen MC, et al. Sutureless securement device reduces complications of peripherally inserted central venous catheters. Journal of Vascular and Interventional Radiology. 2002;13(1):77–81. [PubMed: 11788698].
4.7. Рекомендуем взрослым пациентам при состояниях при ХБП-5 не проводить парентеральной антимикробной профилактики перед введением или регулярно во время использования катетера для гемодиализа для предотвращения колонизации катетера или инфекции кровотока.
Уровень достоверности доказательств II, уровень убедительности рекомендаций B
Комментарии. Пероральные, парентеральные антибактериальные или противогрибковые средства не уменьшают инцидентности бактериемии среди взрослых. Профилактическое использование антибиотика служит независимым показателем риска для развития резистентных форм.
Ljungman P, Hägglund H, Björkstrand B, Lönnqvist B, Ringdén O. Peroperative teicoplanin for prevention of gram-positive infections in neutropenic patients with indwelling central venous catheters: a randomized, controlled study. Support Care Cancer. 1997 Nov;5(6):485–488.
McKee R, Dunsmuir R, Whitby M et al. Does antibiotic prophylaxis at the time of catheter insertion reduce the incidence of catheter-related sepsis in intravenous nutrition? Journal of Hospital Infection. 1985;6:419–425.
Ranson MR, Oppenheim BA, Jackson A et al. Double-blind placebo controlled study of vancomycin prophylaxis for central venous catheter insertion in cancer patients. Journal of Hospital Infection. 1990;15:95–102.
van de Wetering MD, van Woensel JB. Prophylactic antibiotics for preventing early central venous catheter Gram positive infections in oncology patients. Cochrane Database Syst Rev. 2007 (1)CD003295.
5. Манипуляции при уходе за катетером для диализа
5.1. Рекомендуем медицинскому персоналу при работе с катетером для гемодиализа проводить гигиеническую обработку рук, включающую применение кожного антисептика на спиртовой основе, без предварительного мытья рук мылом и водой.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. При работе с катетером для гемодиализа в процессе его использования во время процедуры допустимо использование чистых нестерильных перчаток (при условии обязательной обработки рук антисептиком перед надеванием нестерильных перчаток).
Fluk R, Kumwenda MJ, Prevention of catheter related infections. Guideline 5.1, in Vascular access for haemodialysis. 2011, UK Renal Association.
Maiwald M, Chan ES. The forgotten role of alcohol: a systematic review and meta-analysis of the clinical efficacy and perceived role of chlorhexidine in skin antisepsis. PLoS ONE 2012;7(9):e44277.
O’Horo JC, Silva GL, Munoz-Price LS, Safdar N. The efficacy of daily bathing with chlorhexidine for reducing healthcare associated bloodstream infections: a meta analysis. Infect Control Hosp Epidemiol 2012;33(3):257–267.
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
5.2. Рекомендуем обязательно использовать асептическую технику при каждой манипуляции с катетером для гемодиализа.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Соединение, разъединение и манипуляции с катетером для гемодиализа должны производиться обученным персоналом с применением асептической техники и при наличии хирургической маски и шапочки у пациента. В частности, два медицинских работника необходимы для подключения пациента с ЦВК для гемодиализа к аппарату искусственная почка с целью поддержания асептической техники. Уровень инфицирования катетеров для гемодиализа повышается, когда манипуляции с катетером осуществляются недостаточно обученным персоналом.
Allon M, Depner TA, Radeva M, Bailey J, Beddhu S, Butterly D, Coyne DW, Gassman JJ, Kaufman AM, Kaysen GA, Lewis JA, Schwab SJ; HEMO Study Group: Impact of dialysis dose and membrane on infection-related hospitalization and death: Results of the HEMO Study. J AmSoc Nephrol, 14:1863–1870, 2003.
Aslam S, Vaida F, Ritter M, Mehta RL. Systematic review and metaanalysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol: JASN. 2014;25(12):2927–2941.
Blot K, Bergs J, Vogelaers D, et al. Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect Dis. 2014;59:96–105. Doi: 10.1093/cid/ciu239.
Carrer S, Bocchi A, Bortolotti M, et al. Effect of different sterile barrier precautions and central venous catheter dressing on the skin colonization around the insertion site. Minerva Anestesiol. 2005;71(5):197–206. [PubMed: 15834348].
Hymes JL, Mooney A, Van Zandt C, Lynch L, Ziebol R, Killion D. Dialysis Catheter-Related Bloodstream Infections: A Cluster-Randomized Trial of the ClearGuard HD Antimicrobial Barrier Cap. Am J Kidney Dis. 2017;69(2):220–227.
Lemaire X, Morena M, Leray-Moragues H et al. Analysis of risk factors for catheter-related bacteremia in 2000 permanent dual catheters for hemodialysis. Blood Purif 2009;28:21–28.
Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clinic proceedings Mayo Clinic. 2006; 81(9):1159–1171. [PubMed: 16970212].
McCann M, Moore ZE. Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database Systematic Review 2010; 20(1):CD00689.
McLure HA, Talboys CA, Yentis SM, Azadian BS. Surgical face masks and downward dispersal of bacteria. Anaesthesia. 1998 Jul;53(7):624–626.
Mermel LA, Maki DG. Infectious complications of Swan-Ganz pulmonary artery catheters. Pathogenesis, epidemiology, prevention, and management. Am J Respir Crit Care Med. 1994; 149(4 Pt 1):1020–1036. [PubMed: 8143037].
Oliver MJ, Callery SM, Thorpe KE et al. Risk of bacteraemia from temporary hemodialysis catheters by site of insertion and duration of use: A prospective study. Kidney Int 2000; 58:2543–2545, 4. Lee T, Barker J, Allon M. Tunneled catheters in hemodialysis patients: reasons and subsequent outcomes. Am J Kidney Dis 2005;46:501–508.
Quittnat Pelletier F, Joarder M, Poutanen SM, Lok CE. Evaluating approaches for the diagnosis of hemodialysis catheter-related bloodstream infections. Clin J Am Soc Nephrol: CJASN.2016;11(5):847–854.
Rosenblum A, Wang W, Ball LK, Latham C, Maddux FW, Lacson E, Jr. Hemodialysis catheter care strategies: a cluster-randomized quality improvement initiative. Am J Kidney Dis. 2014;63(2):259–267.
Thomson P, Stirling C, Traynor J, Morris S, Mactier R. A prospective observational study of catheter-related bacteraemia and thrombosis in a haemodialysis cohort: univariate and multivariate analyses of risk associations. Nephrol Dial Transplant 2010; 25(5):1596-60.
Vats HS. Complications of catheters: tunneled and nontunneled. Adv Chronic Kidney Dis, 2012;19:188–194.
Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39(3):309–317. [PubMed: 15306996].
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
5.3. Предлагаем проводить осмотр места выхода катетера перед каждой процедурой диализа или манипуляцией с катетером.
Уровень достоверности доказательств II, уровень убедительности рекомендаций B
Комментарии. Контролируйте места выхода катетера визуально при смене повязки или при пальпации через неповрежденную повязку на регулярной основе в зависимости от клинической ситуации или конкретного пациента. Место выхода катетера должно быть осмотрено опытным персоналом перед каждой процедурой гемодиализа на предмет правильного положения катетера, отсутствия инфекции до открытия доступа к катетеру. Если у пациентов отмечается болезненность в месте выхода ЦВК, лихорадка без очевидного источника или другие проявления, предполагающие местное воспаление или инфекцию кровотока, повязка должна быть удалена, чтобы позволить тщательное обследовать место выхода катетера.
Rasero L, Degl'Innocenti M, Mocali M, et al. [Comparison of two different protocols on change of medication in central venous catheterization in patients with bone marrow transplantation: results of a randomized multicenter study]. Assist Inferm Ric. 2000;19(2):112–119. [PubMed: 11107366].
Timsit JF, Schwebel C, Bouadma L, et al. Chlorhexidine-impregnated sponges and less frequent dressing changes for prevention of catheter-related infections in critically ill adults: a randomized controlled trial. JAMA. 2009;301(12):1231–1241. [PubMed: 19318651].
5.4. Рекомендуем использовать стерильную марлевую повязку или стерильную прозрачную полупроницаемую повязку для надежной фиксации катетера для гемодиализа, минимизации механических повреждений кожи и защиты раны места выхода катетера от контаминации извне.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Если у пациента диафорез или выделения из места выхода катетера, используйте марлевую повязку, которая должна сменяться через каждые 48 часов. Смена прозрачной полупроницаемой повязки, производится, согласно рекомендациям производителя, по крайней мере каждые 7 дней.
Beathard GA, Urbanes A Infection associated with tunneled hemodialysis catheters. Semin Dial. 2008 Nov-Dec;21(6):528–538. Doi: 10.1111/j.1525-139X.2008.00497.x. Epub 2008 Sep 24.
Benhamou E, Fessard E, Com-Nougué C et al. Less frequent catheter dressing changes decrease local cutaneous toxicity of high-dose chemotherapy in children, without increasing the rate of catheter-related infections: results of a randomised trial. Bone marrow transplantation. 2002;29 653.
Bijma R, Girbes AR, Kleijer DJ, Zwaveling JH. Preventing central venous catheter-related infection in a surgical intensive-care unit. Infect Control Hosp Epidemiol. 1999; 20(9):618–620. [PubMed: 10501261].
Gilles D, O’Riordan L, Carr D et al. Gauze and tape and transparent polyurethane dressings for central venous catheters. Cochrane Database Systematic Review 2003;4:CD00382.
Ho KM, Litton E. Use of chlorhexidine-impregnated dressing to prevent vascular and epidural catheter colonization and infection: a meta-analysis. J Antimicrob Chemother 2006;58:281–287.
Hoffmann KK, Weber DJ, Samsa GP, Rutala WA. Transparent polyurethane film as an intravenous catheter dressing A meta-analysis of the infection risks. Jama. 1992; 267(15):2072– 2076. [PubMed: 1532429].
Le Corre I, Delorme M, Cournoyer S. A prospective, randomized trial comparing a transparent dressing and a dry gauze on the exit site of long term central venous catheters of hemodialysis patients. The Journal of Vascular Access. 2003;4:56–61.
Madeo M, Martin CR, Turner C, Kirkby V, Thompson DR. A randomized trial comparing Arglaes (a transparent dressing containing silver ions) to Tegaderm (a transparent polyurethane dressing) for dressing peripheral arterial catheters and central vascular catheters. Intensive Crit Care Nurs. 1998;14(4):187–191. [PubMed: 9849245].
Maki DG, Stolz SS, Wheeler S, Mermel LA. A prospective, randomized trial of gauze and two polyurethane dressings for site care of pulmonary artery catheters: implications for catheter management. Crit Care Med. 1994; 22(11):1729–1737. [PubMed: 7956275] 136.
McCann M and Moore Zena EH (2010) Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database of Systematic Reviews. Doi: 10.1002/14651858.CD006894.pub2.
Olson K, Rennie RP, Hanson J et al. Evaluation of a no-dressing intervention for tunneled central venous catheter exit sites. Journal of Infusion Nursing. 2004;27:37–44.
Rasero L, Degl'Innocenti M, Mocali M, et al. [Comparison of two different protocols on change of medication in central venous catheterization in patients with bone marrow transplantation: results of a randomized multicenter study]. Assist Inferm Ric. 2000;19(2):112–119. [PubMed: 11107366].
Rickard C and Ray-Barruel G, Systematic Review of Infection Control Literature Relating to Intravascular Devices. 2009, Griffith University.1–206.
Ruschulte H, Franke M, Gastmeier P, et al. Prevention of central venous catheter related infections with chlorhexidine gluconate impregnated wound dressings: a randomized controlled trial. Ann Hematol 2009;88:267–272.
Timsit JF, Schwebel C, Bouadma L, et al. Chlorhexidine-impregnated sponges and less frequent dressing changes for prevention of catheter-related infections in critically ill adults: a randomized controlled trial. JAMA. 2009;301(12):1231–1241. [PubMed: 19318651].
5.5. Предлагаем проводить смену повязки центрального венозного катетера на регулярной основе, ее следует менять как можно раньше, если она не чистая или порвана.
Уровень достоверности доказательств II, уровень убедительности рекомендаций B
Комментарии. В настоящее время нет рекомендаций относительно необходимости какой-либо повязки на хорошо зажженных участках места выхода туннельных центральных венозных катетеров для гемодиализа.
Gillies D, Carr D, Frost J et al. Gauze and tape and transparent polyurethane dressings for central venous catheters Cochrane Database of Systematic Reviews 2003:CD003827.
Harwood L, Wilson B, Thompson B et al. Predictors of hemodialysis central venous catheter exit-site infections. Cannt Journal. 2008;18:26–35.
Hoffmann KK, Weber DJ, Samsa GP, Rutala WA Transparent polyurethane film as an intravenous catheter dressing. A meta-analysis of the infection risks. JAMA. 1992 Apr 15;267(15):2072–2076.
Le Corre I, Delorme M, and Cournoyer S. A prospective, randomized trial comparing a transparent dressing and a dry gauze on the exit site of long term central venous catheters of hemodialysis patients. The journal of vascular access. 2003;4:56.
Maki DG, Ringer M.Evaluation of dressing regimens for prevention of infection with peripheral intravenous catheters. Gauze, a transparent polyurethane dressing, and an iodophor-transparent dressing. JAMA. 1987 Nov 6;258(17):2396–2403.
5.6. Рекомендуем использовать асептическую технику при смене повязки центрального венозного катетера.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Смена повязки происходит с заменой перчаток. Перед проведением манипуляции медицинский работник проводит гигиеническую обработку рук, надевает нестерильные перчатки, снимает повязку в месте ведения ЦВК, снимает нестерильные перчатки. Далее медицинский работник обрабатывает руки антисептиком, надевает стерильные перчатки, проводит обработку кожи вокруг катетера бесконтактным способом, наклеивает стерильную повязку на высохший кожный покров пациента.
СанПиН 2.1.3.2630-10 «Санитарно-эпидемиологические требования к организациям, осуществляющим медицинскую деятельность» (с изменениями на 10.06.2016).
McCann M and Moore Zena EH (2010) Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database of Systematic Reviews. Doi: 10.1002/14651858.CD006894.pub2.
Rasero L, Degl'Innocenti M, Mocali M, et al. [Comparison of two different protocols on change of medication in central venous catheterization in patients with bone marrow transplantation: results of a randomized multicenter study]. Assist Inferm Ric. 2000;19(2):112–119. [PubMed: 11107366].
5.7. Рекомендуем использовать только одноразовые стерильные медицинские изделия при работе с катетером для гемодиализа.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Заглушки катетеров для диализа служат частым источником обсеменения, особенно при длительной катетеризации. Использование двух новых заглушек снижает риск катетер-ассоциированной инфекции и бактериемии.
Blot K, Bergs J, Vogelaers D, et al. Prevention of central line-associated bloodstream infections through quality improvement interventions: a systematic review and meta-analysis. Clin Infect Dis. 2014;59:96–105. Doi: 10.1093/cid/ciu239.
Bonawitz SC, Hammell EJ, Kirkpatrick JR. Prevention of central venous catheter sepsis: A prospective randomized trial. Am Surg. 1991;57:618–623.
Brunelli SM, Van Wyck DB, Njord L, Ziebol RJ, Lynch LE, Killion DP. Cluster-randomized trial of devices to prevent catheter-related bloodstream infection. J Am Soc Nephrol: JASN. 2018;29(4):1336–1343.
Halpin DP, O'Byrne P, McEntee G, Hennessy TP, Stephens RB. Effect of a betadine connection shield on central venous catheter sepsis. Nutrition. 1991 Jan-Feb;7(1):33–34.
McCann M, Moore ZE. Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database Systematic Review 2010;20(1):CD00689.
Raad II, Hohn DC, Gilbreath BJ, et al. Prevention of central venous catheter-related infections by using maximal sterile barrier precautions during insertion. Infect Control Hosp Epidemiol. 1994;15:231–238. [PubMed: 8207189].
Rosenblum A, Wang W, Ball LK, Latham C, Maddux FW, Lacson E, Jr. Hemodialysis catheter care strategies: a cluster-randomized quality improvement initiative. Am J Kidney Dis. 2014;63(2):259–267.
Segura M, Alvarez-Lerma F, Tellado JM, Jiménez-Ferreres J, Oms L, Rello J, Baró T, Sánchez R, Morera A, Mariscal D, Marrugat J, Sitges-Serra A. A clinical trial on the prevention of catheter-related sepsis using a new hub model. Ann Surg. 1996 Apr;223(4):363–369.
Silva TN, de Marchi D, Mendes ML et al. Approach to prophylactic measures for central venous catheter-related infections in hemodialysis: a critical review. Hemodial Int 2014;18:15–23.
Weaver SJ, Lubomksi LH, Wilson RF, Pfoh ER, Martinez KA, Dy SM. Promoting a culture of safety as a patient safety strategy: a systematic review. Ann Intern Med 2013;158(5 pt 2):369– 374.
5.8. Предлагаем обрабатывать спиртосодержащим антисептиком порт (конектор) катетера для гемодиализа перед и после каждой процедуры диализа.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Tordoir J, Canaud B, Haage P et al. EBPG on Vascular Access. Nephrology Dialysis Transplantation. 2007;22:ii88–117.
Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012;120:179–184
5.9. Рекомендуем использовать антибактериальные мази или кремы (повидон–йод или [бацитрацин/грамицидин/полимиксин B] полиспорин) в месте выхода туннелированного катетера для гемодиализа, если они не взаимодействует с материалом катетера, после введения катетера и в конце каждой процедуры диализа до полного заживления места введения.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. В соответствии с рекомендациями производителя следует прекратить их применение после заживления. Не следует применять антимикробные мази или кремы на местах введения катетера под повязку, фиксирующую нетуннелированный катетер в отделении интенсивной терапии. Рекомендации больным ОПП, находящимся на лечении вне реанимации или интенсивной терапии, отсутствуют.
Battistella M, Bhola C, Lok CE. Long-term follow-up of the Hemodialysis Infection Prevention with Polysporin Ointment (HIPPO) Study: a quality improvement report. Am J Kidney Dis (in press).
Beathard GA, Urbanes A Infection associated with tunneled hemodialysis catheters. Semin Dial. 2008 Nov-Dec;21(6):528-38. doi: 10.1111/j.1525-139X.2008.00497.x. Epub 2008 Sep 24.
Bernardini J, Bender F, Florio T, Sloand J, Palmmontalbano L, Fried L, Piraino B. Randomized, double-blind trial of antibiotic exit site cream for prevention of exit site infection in peritoneal dialysis patients.J Am Soc Nephrol. 2005. Feb;16(2):539–545. Epub 2004 Dec 29.
Casewell MW.The nose: an underestimated source of Staphylococcus aureus causing wound infection. J Hosp Infect. 1998 Sep;40 Suppl B:S3–11. Review.
Chu KH, Choy WY, Cheung CC, Fung KS, Tang HL, Lee W, Cheuk A, Yim KF, Chan WH, Flowers RH 3rd, Schwenzer KJ, Kopel RF, Fisch MJ, Tucker SI, Farr BM. Efficacy of an attachable subcutaneous cuff for the prevention of intravascular catheter-related infection A randomized, controlled trial. Jama. 1989;261(6):878–883. [PubMed: 2492354].
Fong IW. Prevention of haemodialysis and peritoneal dialysis catheter related infection by topical povidone-iodine. Postgrad Med J. 1993;69(Suppl 3):S15–S17. [PubMed: 8290450].
Fukunaga A, Naritaka H, Fukaya R, Tabuse M, Nakamura T. Povidone-iodine ointment and gauze dressings associated with reduced catheter-related infection in seriously ill neurosurgical patients. Infect Control Hosp Epidemiol. 2004;25(8):696–698. [PubMed: 15357164].
Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
Hill RL, Fisher AP, Ware RJ, Wilson S, Casewell MW. Mupirocin for the reduction of colonization of internal jugular cannulae–a randomized controlled trial. J Hosp Infect 1990;15:311–321.
James MT, Conley J, Tonelli M et al. Meta-analysis: Antibiotics for prophylaxis against hemodilaysis catheter related infections. Ann Intem Med 2008;148:596–605.
Johnson DW, MacGinley R, Kay TD, et al. A randomized controlled trial of topical exit site mupirocin application in patients with tunnelled, cuffed haemodialysis catheters. Nephrol Dial Transplant. 2002;17(10):1802–1807. [PubMed: 12270988].
Johnson DW, van Eps C, Mudge DW et al. Randomized, controlled trial of topical exit-site application of honey (Medihoney) versus mupirocin for the prevention of catheter-associated infections in hemodialysis patients. Journal of the American Society of Nephrology. 2005;16:1456–1462.
Levin A, Mason AJ, Jindal KK, Fong IW, Goldstein MB. Prevention of hemodialysis subclavian vein catheter infections by topical povidone-iodine. Kidney Int. 1991;40:934–938. [PubMed: 1762298].
Lok CE, Stanley KE, Hux JE et al. Hemodialysis infection prevention with polysporin ointment. Journal of the American Society of Nephrology. 2003;14:169–179.
Maki DG, Band JD. A comparative study of polyantibiotic and iodophor ointments in prevention of vascular catheter-related infection. Am J Med. 1981;70(3):739–744. [PubMed: 6259941] 149.
Maki DG, Stolz SS, Wheeler S, Mermel LA. A prospective, randomized trial of gauze and two polyurethane dressings for site care of pulmonary artery catheters: implications for catheter management. Crit Care Med 1994;22:1729–1737.
Marschall J, Mermel LA, Classen D, et al. Strategies to prevent central lineassociated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol 2008;29(Suppl 1):S22–30.
McCann M, Moore ZE. Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD006894.
Miller MA, Dascal A, Portnoy J, Mendelson J. Development of mupirocin resistance among methicillin-resistant Staphylococcus aureus after widespread use of nasal mupirocin ointment. Infect Control Hosp Epidemiol. 1996 Dec;17(12):811–813.
Pratt RJ, Pellowe CM, Wilson JA, et al. epic2: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 2007;65 (Suppl 1):S1–64.
Rabindranath KS, Bansal T, Adams J et al. Systematic review of antimicrobials for the prevention of haemodialysis catheter-related infections. Nephrology Dialysis Transplantation. 2009;24:
3763–3774.
Sesso R, Barbosa D, Leme IL et al. Staphylococcus aureus prophylaxis in hemodialysis patients using central venous catheter: effect of mupirocin ointment. J Am Soc Nephrol 1998;9:1085–1092.
Tacconelli E, Carmeli Y, Aizer A et al. Mupirocin prophylaxis to prevent Staphylococcus aureus infection in patients undergoing dialysis: a meta-analysis. Clin Infect Dis 2003;37:1629–1638.
Zakrzewska-Bode A, Muytjens HL, Liem KD, Hoogkamp-Korstanje JA. Mupirocin resistance in coagulase-negative staphylococci, after topical prophylaxis for the reduction of colonization of central venous catheters. J Hosp Infect. 1995;31(3):189–193. [PubMed: 8586787].
5.10. Рекомендуем снижать колонизацию S. aureus введением интраназально антибактериального средства больным при состояниях при ХБП-5 с туннелированным катетером, используемым в качестве сосудистого доступа.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Назальное носительство S. aureus – частое явление, поэтому пациентам необходимо применять хирургические маски, а не только сестерам при манипуляциях с катетером для диализа. Бактериальная деколонизация S. aureus интраназально мупироцином значительно снизила частоту бактериемии у больных с туннелированным катетером, у пациентов при состояниях при ХБП-5.
Battistella M, Bhola C, Lok CE. Long-term follow-up of the Hemodialysis Infection Prevention with Polysporin Ointment (HIPPO) Study: a quality improvement report. Am J Kidney Dis. 2011 Mar;57(3):432–441. Doi: 10.1053/j.ajkd.2010.10.009. Epub 2011 Jan 8.
Beathard GA. Urbanes A Infection associated with tunneled hemodialysis catheters. Semin Dial. 2008 Nov-Dec;21(6):528–538. Doi: 10.1111/j.1525-139X.2008.00497.x. Epub 2008 Sep 24.
Bloom BS, Fendrick AM, Chernew ME, Patel P. Clinical and economic effects of mupirocin calcium on preventing Staphylococcus aureus infection in hemodialysis patients: a decision analysis. Am J Kidney Dis. 1996 May;27(5):687–694.
Casewell MW.The nose: an underestimated source of Staphylococcus aureus causing wound infection. J Hosp Infect. 1998 Sep;40 Suppl B:S3–11. Review.
Danese MD, Griffiths RI, Dylan M, Yu HT, Dubois R, Nissenson AR. Mortality differences among organisms causing septicemia in hemodialysis patients. Hemodial Int. 2006 Jan;10(1):56–62.
Hill RL, Fisher AP, Ware RJ, Wilson S, Casewell MW. Mupirocin for the reduction of colonization of internal jugular cannulae–a randomized controlled trial. J Hosp Infect 1990;15:311–321.
Huang SS, Septimus E, Kleinman K, Moody J, Hickok J, Avery TR, Lankiewicz J, Gombosev A, Terpstra L, Hartford F, Hayden MK, Jernigan JA, Weinstein RA, Fraser VJ, Haffenreffer K, Cui E, Kaganov RE, Lolans K, Perlin JB, Platt R; CDC Prevention Epicenters Program; AHRQ DECIDE Network and Healthcare-Associated Infections Program.
James MT, Conley J, Tonelli M et al. Meta-analysis: Antibiotics for prophylaxis against hemodilaysis catheter related infections. Ann Intem Med 2008;148:596–605.
Johnson LB, Jose J, Yousif F, Pawlak J, Saravolatz LD. Prevalence of colonization with community-associated methicillin-resistant Staphylococcus aureus among end-stage renal disease patients and healthcare workers. Infect Control Hosp Epidemiol. 2009 Jan;30(1):4–8. Doi: 10.1086/592983.
Kluytmans JA, Manders MJ, van Bommel E, Verbrugh H.E limination of nasal carriage of Staphylococcus aureus in hemodialysis patients. Infect Control Hosp Epidemiol. 1996 Dec;17(12):793–797.
Lok CE, Mokrzycki MH. Prevention and management of catheter-related infection in hemodialysis patients. Kidney Int 2011;79:587–598.
Lok CE, Stanley KE, Hux JE, Richardson R, Tobe SW, Conly J. Hemodialysis infection prevention with polysporin ointment. J Am Soc Nephrol 2003;14:169–179.
McCann M and Moore Zena EH (2010) Interventions for preventing infectious complications in haemodialysis patients with central venous catheters. Cochrane Database of Systematic Reviews, Doi: 10.1002/14651858.CD006894.pub2.
Mermel LA, Farr BM, Sherertz RJ, Raad II, O'Grady N, Harris JS, Craven DE; Infectious Diseases Society of America; American College of Critical Care Medicine; Society for Healthcare Epidemiology of America. Guidelines for the management of intravascular catheter-related infections. Clin Infect Dis. 2001 May 1;32(9):1249–1272. Epub 2001 Apr 3.
Nissenson AR, Dylan ML, Griffiths RI, Yu HT, Dean BB, Danese MD, Dubois RW.Clinical and economic outcomes of Staphylococcus aureus septicemia in ESRD patients receiving hemodialysis. Am J Kidney Dis. 2005 Aug;46(2):301–308.
Rabindranath KS, Bansal T, Adams J et al. Systematic review of antimicrobials for the prevention of haemodialysis catheter-related infections. Nephrology Dialysis Transplantation. 2009;24:3763–3774.
Sesso R, Barbosa D, Leme IL et al. Staphylococcus aureus prophylaxis in hemodialysis patients using central venous catheter: effect of mupirocin ointment. J Am Soc Nephrol 1998;9:1085–1092.
Tacconelli E, Carmeli Y, Aizer A, Ferreira G, Foreman MG, D'Agata EM Mupirocin prophylaxis to prevent Staphylococcus aureus infection in patients undergoing dialysis: a meta-analysis. Clin Infect Dis. 2003 Dec 15;37(12):1629–1638. Epub 2003 Nov 20.
von Eiff C, Jansen B, Kohnen W, Becker K Infections associated with medical devices: pathogenesis, management and prophylaxis. Drugs. 2005;65(2):179–214.
5.11. Рекомендуем при эксплуатации центрального венозного катетера для гемодиализа в медицинскую документацию вносить данные о состоянии катетера и кожных покровов вокруг места выхода катетера, наличии признаков локальной воспалительной реакции (покраснения, экссудата, болезненности, отечности), нарушении целостности швов в растворе для внутрипросветной экспозиции во время каждой процедуры диализа, информацию о смещениях, удалении/обмене катетера.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Ma IW, Brindle ME, Ronksley PE, Lorenzetti DL, Sauve RS, Ghali WA. Use of simulation-based education to improve outcomes of central venous catheterization: a systematic review and meta-analysis. Acad Med 2011;86(9):1137–1147.
Safdar N, Abad C. Educational interventions for prevention of healthcare-associated infection: a systematic review. Crit Care Med 2008;36(3):933–940.
Aboelela SW, Stone PW, Larson EL. Effectiveness of bundled behavioural interventions to control healthcare-associated infections: a systematic review of the literature. J Hosp Infect 2007;66(2):101–108.
5.12. Рекомендуем не погружаться с катетером для гемодиализа в воду. Душ может быть разрешен, если есть возможность принять меры уменьшения вероятности инфицирования катетера (например, катетер защищен непроницаемой повязкой или устройством во время принятия душа).
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Robbins J, Cromwell P, Korones DN. Swimming and central venous catheter-related infections in the child with cancer. J Pediatr Oncol Nurs. 1999;16(1):51–56. [PubMed: 9989017].
Howell PB, Walters PE, Donowitz GR, Farr BM. Risk factors for infection of adult patients with cancer who have tunnelled central venous catheters. Cancer. 1995;75(6):1367–1375. [PubMed: 7882288]
Ivy DD, Calderbank M, Wagner BD, et al. Closed-hub systems with protected connections and the reduction of risk of catheter-related bloodstream infection in pediatric patients receiving intravenous prostanoid therapy for pulmonary hypertension. Infect Control Hosp Epidemiol. 2009;30(9):823–829. [PubMed: 19637961]
6. Манипуляции для профилактики и лечения дисфункции катетера для диализа
6.1. Предлагаем проводить промывание центрального венозного катетера для обеспечения и поддержания его функционирования.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Для промывания используют стерильный 0,9%-ный раствор натрия хлорида в количестве не менее двух объемов заполнения просвета катетера. Использовать флаконы с раствором только индивидуально. Промывать катетер необходимо сразу же после введения ЦВК, перед и после процедуры экстракорпорального диализа, до и после забора крови из катетера.
Abi-Said D, Raad I, Umphrey J, et al. Infusion therapy team and dressing changes of central venous catheters. Infect Control Hosp Epidemiol. 1999;20(2):101–105. [PubMed: 10064212].
Aboelela SW, Stone PW, Larson EL. Effectiveness of bundled behavioural interventions to control healthcare-associated infections: a systematic review of the literature. J Hosp Infect 2007;66(2):101–108.
Bosma TL, Jewesson PJ. An infusion program resource nurse consult service: our experience in a major Canadian teaching hospital. J Infus Nurs. 2002;25(5):310–315. [PubMed: 12355056].
Brunelle D. Impact of a dedicated infusion therapy team on the reduction of catheter-related nosocomial infections. J Infus Nurs. 2003;26(6):362–366. [PubMed: 14624176].
Safdar N, Abad C. Educational interventions for prevention of healthcare-associated infection: a systematic review. Crit Care Med 2008;36 (3):933–940.
6.2. Полагаем, что количество раствора для внутрипросветной экспозиции не должно превышать одного объема заполнения просвета катетера для гемодиализа.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Растворы для внутрипросветной экспозиции для катетера содержат либо антибиотик, либо антисептик, либо антикоагулянт, либо другое вещество или их комбинации, способствуют предотвращению образования биопленки, колонизации катетера, уничтожению бактерий, содержащихся в биопленке. Идеальный раствор для внутрипросветной экспозиции для профилактики и лечения дисфункции и инфекции катетера не известен.
Bosma JW, Siegert CE, Peerbooms PG et al. Reduction of biofilm formation with trisodium citrate in haemodialysis catheters: a randomized controlled trial. Nephrol Dial Transplant 2010;25:1213–1217.
Broom JK, Krishnasamy R, Hawley CM, Playford EG, Johnson DW. A randomised controlled trial of Heparin versus EthAnol Lock THerapY for the prevention of Catheter Associated infecTion in Haemodialysis patients--the HEALTHY-CATH trial. BMC Nephrol. 2012 Nov 2;13:146. Doi: 10.1186/1471-2369-13-146.
Buturovic J, Ponikvar R, Kandus A, Boh M, Klinkmann J, Ivanovich P. Filling hemodialysis catheters in the interdialytic period: heparin versus citrate versus polygeline: a prospective randomized study. Artif Organs 1998;22:945–947.
Chapla K, Oza-Gajera BP, Yevzlin AS, Shin JI, Astor BC, Chan MR. Hemodialysis catheter locking solutions and the prevention of catheter dysfunction: a meta-analysis. J Vasc Access. 2015;16(2):107–112
Correa Barcellos F, Pereira Nunes B, Jorge Valle L, Lopes T, Orlando B, Scherer C, et al. Comparative effectiveness of 30 % trisodium citrate and heparin lock solution in preventing infection and dysfunction of hemodialysis catheters: a randomized controlled trial (CITRIM trial). Infection. 2017;45(2):139–145.
Fernández-Gallego J, Martín M, Gutiérrez E, Cobelo C, Frías P, Jironda C, Hidalgo P, Jiménez T.Filiopoulos V, Hadjiyannakos D, Koutis I et al. Approaches to prolong the use of uncuffed hemodialysis catheters: results of a randomized trial. Am J Nephrol 2011;33:260–268.
Grudzinski L, Quinan P, Kwok S, Pierratos A. Sodium citrate 4% locking solution for central venous dialysis catheters--an effective, more cost-efficient alternative to heparin. Nephrol Dial Transplant. 2007 Feb;22(2):471–476. Epub 2006 Oct 25.
Han X, Yang X, Huang B, Yuan L, Cao Y. Low-dose versus high-dose heparin locks for hemodialysis catheters: a systematic review and meta-analysis. Clin Nephrol. 2016 Jul;86(7):1–-8. Doi: 10.5414/CN108701.
Hemmelgarn BR, Manns BJ, Soroka SD, Levin A, MacRae J, Tennankore K, Wilson JS, Weaver RG, Ravani P, Quinn RR, Tonelli M, Kiaii M, Mossop P, Scott-Douglas N. Effectiveness and Cost of Weekly Recombinant Tissue Plasminogen Activator Hemodialysis Catheter Locking Solution. Clin J Am Soc Nephrol. 2018 Mar 7;13(3):429–435. Doi: 10.2215/CJN.08510817. Epub 2018 Jan 15.
Hemmelgarn BR, Moist L, Pilkey RM, Lok C, Dorval M, Tam PY, Berall MJ, LeBlanc M, Toffelmire EB, Manns BJ, Scott-Douglas N; Canadian Hemodialysis Catheter Working Group. Prevention of catheter lumen occlusion with rT-PA versus heparin (Pre-CLOT): study protocol of a randomized trial [ISRCTN35253449]. BMC Nephrol. 2006 Apr 11;7:8.
Hemmelgarn BR, Moist LM, Lok CE, Tonelli M, Manns BJ, Holden RM, LeBlanc M, Faris P, Barre P, Zhang J, Scott-Douglas N; Prevention of Dialysis Catheter Lumen Occlusion with rt-PA versus Heparin Study Group Prevention of dialysis catheter malfunction with recombinant tissue plasminogen activator. N Engl J Med. 2011 Jan 27;364(4):303–12. Doi: 10.1056/NEJMoa1011376.
Hermite L, Quenot JP, Nadji A, Barbar SD, Charles P-E, Hamet M, et al. Sodium citrate versus saline catheter locks for non-tunneled hemodialysis central venous catheters in critically ill adults: a randomized controlled trial. Intensive Care Med 2012;38:279–285.
Holley JL, Bailey S. Catheter lock heparin concentration: effects on tissue plasminogen activator use in tunneled cuffed catheters. Hemodial Int. 2007 Jan;11(1):96–98.
Hendrickx L, Kuypers D, Evenepoel P, Maes B, Messiaen T, Vanrenterghem Y. A comparative prospective study on the use of low concentrate citrate lock versus heparin lock in permanent dialysis catheters. Int J Artif Organs 2001;24:208–211.
Jaffer Y, Selby NM, Taal MW et al. A meta-analysis of hemodialysis catheter locking solutions in the prevention of catheter-related infection. American journal of kidney diseases. 2008;51:233–241.
Kethireddy S, Safdar N. Urokinase lock or flush solution for prevention of bloodstream infections associated with central venous catheters for chemotherapy: a meta-analysis of prospective randomized trials. J Vasc Access. 2008. Jan-Mar;9(1):51–57.
Lee T, Lok C, Vazquez M et al. Minimizing hemodialysis catheter dysfunction: an ounce of prevention. Int J Nephrol 2012; 2012:170857.
Lok CE, Mokrzycki MH. Prevention and management of catheter-related infection in hemodialysis patients. Kidney Int 2011;79:587–598.
Lok CE, Appleton D, Bhola C, Khoo B, Richardson RM. Trisodium citrate 4% – an alternative to heparin capping of haemodialysis catheters. Nephrol Dial Transplant. 2007 Feb;22(2):477–483. Epub 2006 Oct 2.
Macrae JM, Dojcinovic I, Djurdjev O, Jung B, Shalansky S, Levin A, Kiaii M. Citrate 4% versus heparin and the reduction of thrombosis study (CHARTS). Clin J Am Soc Nephrol. 2008 Mar;3(2):369–374. Doi: 10.2215/CJN.01760407.
Maiefski M, Rupp ME, Hermsen ED. Ethanol lock technique: review of the literature. Infect Control Hosp Epidemiol. 2009 Nov;30(11):1096–1108. Doi: 10.1086/606162.
Moore CL, Besarab A, Ajluni M, Soi V, Peterson EL, Johnson LE, Zervos MJ , Adams E, Yee J Comparative effectiveness of two catheter locking solutions to reduce catheter-related bloodstream infection in hemodialysis patients. Clin J Am Soc Nephrol. 2014 Jul;9(7):1232–1239. Doi: 10.2215/CJN.11291113. Epub 2014 Jun 26.
Moran J, Sun S, Khababa I, Pedan A, Doss S, Schiller B.A randomized trial comparing gentamicin/citrate and heparin locks for central venous catheters in maintenance hemodialysis patients. Am J Kidney Dis. 2012 Jan;59(1):102–107. Doi: 10.1053/j.ajkd.2011.08.031. Epub 2011 Nov 14.
Moran JE, Ash SR. Committee ACP. Locking solutions for hemodialysis catheters; heparin and citrate – a position paper by ASDIN. Semin Dial 2008;21:490–492.
Oliveira C, Nasr A, Brindle M, Wales PW. Ethanol locks to prevent catheter-related bloodstream infections in parenteral nutrition: a meta-analysis. Pediatrics 2012;129(2):318–329.
Oran NT, Eser I.Impact of heparin locking frequency on preventing temporary dialysis catheter dysfunction in haemodialysis patients. J Ren Care. 2008 Dec;34(4):199–202. Doi: 10.1111/j.1755-6686.2008.00044.x.
Power A, Duncan N, Singh SK, et al. Sodium citrate versus heparin catheter locks for cuffed central venous catheters: a single-center randomized controlled trial. Am J Kidney Dis. 2009;53(6):1034–1041.
Randolph AG, Cook DJ, Gonzales CA, Andrew M. Benefit of heparin in central venous and pulmonary artery catheters: a meta-analysis of randomized controlled trials. Chest. 1998; 113(1):165–171. [PubMed: 9440585].
Rioux JP, De Bortoli B, Quérin S, Déziel C, Troyanov S, Madore F. Measurement of the international normalized ratio (INR) in hemodialysis patients with heparin-locked central venous catheters: evaluation of a novel blood sampling method. J Vasc Access. 2009 Jul–Sep;10(3):180–182.
Shanks RM, Sargent JL, Martinez RM, Graber ML, O'Toole GA. Catheter lock solutions influence staphylococcal biofilm formation on abiotic surfaces. Nephrol Dial Transplant. 2006 Aug;21(8):2247–2255. Epub 2006 Apr 20.
Silva TN, de Marchi D, Mendes ML et al. Approach to prophylactic measures for central venous catheter-related infections in hemodialysis: a critical review. Hemodial Int 2014;18:15–23.
Slobbe L, Doorduijn JK, Lugtenburg PJ et al. Prevention of catheter-related bacteremia with a daily ethanol lock in patients with tunnelled catheters: a randomized, placebo-controlled trial. PLoS One 2010;5:e10840.
Thomas CM, Zhang J, Lim TH, Scott-Douglas N, Hons RB, Hemmelgarn BR; Alberta Kidney Disease Network. Concentration of heparin-locking solution and risk of central venous hemodialysis catheter malfunction. ASAIO J. 2007 Jul-Aug;53(4):485–488.
Venditto M, du Montcel ST, Robert J, Trystam D, Dighiero J, Hue D, Bessette C, Deray G, Mercadal L. Effect of catheter-lock solutions on catheter-related infection and inflammatory syndrome in hemodialysis patients: heparin versus citrate 46% versus heparin/gentamicin. Blood Purif. 2010;29(3):268–273. Doi: 10.1159/000274461.
Weijmer MC, van den Dorpel M, Van de Ven PJ, et al., CITRATE Study Group. Randomized, clinical trial comparison of trisodium citrate 30 and heparin as catheter-locking solution in hemodialysis patients. J Am Soc Nephrol 2005;16:2769–2777.
Winnett G, Nolan J, Miller M, Ashman N. Trisodium citrate 46.7% selectively and safely reduces staphylococcal catheter-related bacteraemia. Nephrol Dial Transplant. 2008 Nov;23(11):3592–3598. Doi: 10.1093/ndt/gfn299. Epub 2008 May 25.
Yaseen O, El-Masri MM, El Nekidy WS et al. Comparison of alteplase (tissue plasminogen activator) high-dose vs. low-dose protocol in restoring hemodialysis catheter function: The ALTEDOSE study. Hemodial. Int. 2013;17:434–440.
Yevzlin AS, Sanchez RJ, Hiatt JG, Washington MH, Wakeen M, Hofmann RM, Becker YT. Concentrated heparin lock is associated with major bleeding complications after tunneled hemodialysis catheter placement. Semin Dial. 2007 Jul–Aug;20(4):351–354.
Zhao Y, Li Z, Zhang L et al. Citrate versus heparin lock for hemodialysis catheters: a systematic review and meta-analysis of randomized controlled trials. Am J Kidney Dis 2014;63:479–490.
6.3. Предлагаем использовать профилактический антибактериальный раствор для внутрипросветной экспозиции взрослым пациентам при состояниях при ХБП-5 с туннелированными центральными венозными катетерами для гемодиализа, при соблюдении асептической техники и наличии анамнеза инфекции кровотока.
Уровень достоверности доказательств II, уровень убедительности рекомендаций B
Комментарии. При лечении бактериемии, ассоциированной с туннелированным катетером для гемодиализа, необходимо использовать либо растворы для внутрипросветной экспозиции с антибиотиками, либо замену по проводнику с парентеральным введением антибиотиков. Если туннелированный катетер для гемодиализа не был удален, посев образцов крови должен быть взят через 1 неделю после завершения лечения.
Abbas SA, Haloob IA, Taylor SL et al. Effect of antimicrobial locks for tunneled hemodialysis catheters on bloodstream infection and bacterial resistance: a quality improvement report. American journal of kidney diseases. 2009;53:492–502.
Al-Hwiesh AK, Abdul-Rahman IS. Successful prevention of tunneled, central catheter infection by antibiotic lock therapy using vancomycin and gentamycin. Saudi J Kidney Dis Transpl. 2007;8(2):239–247. [PubMed: 17496402].
Allon M. Prophylaxis against dialysis catheter-related bacteremia with a novel antimicrobial lock solution. Clin Infect Dis. 2003;36(12):1539–1544. [PubMed: 12802753].
Arechabala MC, Catoni MI, Claro J, et al. Antimicrobial lock solutions for preventing catheter-related infections in haemodialysis. Cochrane Database Syst Rev. 2018;4:CD010597.
Barriga FJ, Varas M, Potin M, et al. Efficacy of a vancomycin solution to prevent bacteremia associated with an indwelling central venous catheter in neutropenic and non-neutropenic cancer patients. Med Pediatr Oncol. 1997;28(3):196–200. [PubMed: 9024516].
Beigi AA, Khansoltani S, Masoudpour H et al. Influence of intralumenal and antibiotic-lock of vancomycin on the rate of catheter removal in the patients with permanent hemodialysis catheters. Saudi Journal of Kidney Diseases and Transplantation. 2010;21:54.
Betjes MG, van Agteren M. Prevention of dialysis catheter-related sepsis with a citratetaurolidine-containing lock solution. Nephrol Dial Transplant. 2004;19(6):1546–1551. [PubMed: 14993498].
Bleyer AJ, Mason L, Russell G et al. A randomized, controlled trial of a new vascular catheter flush solution (minocycline-EDTA) in temporary hemodialysis access. Infect Control Hosp Epidemiol 2005;26:520–524.
Boyce JM.Prevention of central line-associated bloodstream infections in hemodialysis patients. Infect Control Hosp Epidemiol. 2012 Sep;33(9):936–944. Doi: 10.1086/667369. Epub 2012 Jul 23.
Carratala J, Niubo J, Fernandez-Sevilla A, et al. Randomized, double-blind trial of an antibioticlock technique for prevention of gram-positive central venous catheter-related infection in neutropenic patients with cancer. Antimicrob Agents Chemother. 1999;43(9):2200–2204. [PubMed: 10471564].
Daghistani D, Horn M, Rodriguez Z, Schoenike S, Toledano S. Prevention of indwelling central venous catheter sepsis. Med Pediatr Oncol. 1996;26(6):405–408. [PubMed: 8614377].
Dogra GK, Herson H, Hutchison B, et al. Prevention of tunneled hemodialysis catheter-related infections using catheter-restricted filling with gentamicin and citrate: a randomized controlled study. J Am Soc Nephrol. 2002;13(8):2133–2139. [PubMed: 12138146].
Droste JC, Jeraj HA, MacDonald A, Farrington K Stability and in vitro efficacy of antibiotic-heparin lock solutions potentially useful for treatment of central venous catheter-related sepsis. J Antimicrob Chemother. 2003 Apr;51(4):849– 855. Epub 2003 Mar 13.
Geron R, Tanchilevski O, Kristal B.[Catheter lock solution--taurolock for prevention of catheter-related bacteremia in hemodialysis patients]. Harefuah. 2006 Dec;145(12):881–884, 943.
Henrickson KJ, Axtell RA, Hoover SM, et al. Prevention of central venous catheter-related infections and thrombotic events in immunocompromised children by the use of vancomycin/ ciprofloxacin/heparin flush solution: A randomized, multicenter, double-blind trial. J Clin Oncol. 2000; 18(6):1269–1278. [PubMed: 10715297].
Jaffer Y, Selby NM, Taal MW, et al. A meta-analysis of hemodialysis catheter locking solutions in the prevention of catheter-related infection. Am J Kidney Dis 2008;51:233–241.
James MT, Conley J, Tonelli M et al. Meta-analysis: Antibiotics for prophylaxis against hemodilaysis catheter related infections. Ann Intem Med 2008;148:596–605.
Jurewitsch B, Lee T, Park J, Jeejeebhoy K. Taurolidine 2% as an antimicrobial lock solution for prevention of recurrent catheter-related bloodstream infections. JPEN J Parenter Enteral Nutr. 1998;22(4):242–244. [PubMed: 9661127].
Kim SH, Song KI, Chang JW et al. Prevention of uncuffed hemodialysis catheter-related bacteremia using an antibiotic lock technique: a prospective, randomized clinical trial. Kidney Int 2006;69:161–164
Krishnasami Z, Carlton D, Bimbo L et al. Management of hemodialysis catheter-related bacteremia with an adjunctive antibiotic lock solution. Kidney International. 2002;61:1136–1142
Labriola L, Crott R, and Jadoul M. Preventing haemodialysis catheter-related bacteraemia with an antimicrobial lock solution: a meta-analysis of prospective randomized trials. Nephrology Dialysis Transplantation. 2008;23:1666–1672.
Landry D, Braden G Reducing catheter-related infections in hemodialysis patients. Clin J Am Soc Nephrol. 2014 Jul;9(7):1156–1159. Doi: 10.2215/CJN.04700514. Epub 2014 Jun 26.
Landry DL, Braden GL, Gobeille SL et al. Emergence of gentamicin-resistant bacteremia in hemodialysis patients receiving gentamicin lock catheter prophylaxis. Clinical Journal of The American Society of Nephrology: CJASN. 2010;5:1799–1804.
Liu H, Liu H, Deng J, Chen L, Yuan L, Wu Y. Preventing catheter-related bacteremia with taurolidine-citrate catheter locks: a systematic review and meta-analysis. Blood Purif. 2014;37(3):179–187.
Luiz MV, Scavone C, Tzanno C. The CLOCK trial, a double-blinded randomized controlled trial: Trisodium citrate 30% and minocycline 3 mg/mL plus EDTA 30 mg/mL are effective and safe for catheter patency maintenance among CKD 5D patients on hemodialysis. Hemodial Int. 2017;21(2):294–304.
Maki DG, Ash SR, Winger RK et al. Investigators AT. A novel antimicrobial and antithrombotic lock solution for hemodialysis catheters: a multi-center, controlled, randomized trial. Crit Care Med 2011;39:613–620.
Marr KA, Sexton DJ, Conlon PJ et al. Catheter-related bacteremia and outcome of attempted catheter salvage in patients undergoing hemodialysis. Annals of internal medicine. 1997;127: 275–280.
McIntyre CW, Hulme LJ, Taal M, Fluck RJ. Locking of tunneled hemodialysis catheters with gentamicin and heparin. Kidney Int. 2004;66(2):801–805. [PubMed: 15253736].
Mokrzycki MH, Zhang M, Golestaneh L et al. An interventional controlled trial comparing 2 management models for the treatment of tunneled cuffed catheter bacteremia: a collaborative team model versus usual physician-managed care. American journal of kidney diseases. 2006;48:587–595.
Moran JE, Sun S, Khababa I, Pedan A, Doss S, Schiller B. A randomized trial comparing gentamicin-citrate and heparin locks for central venous catheters in maintenance hemodialysis patients. Am J Kidney Dis. 2012;59(1):102–107.
Nori US, Manoharan A, Yee J, Besarab A. Comparison of low-dose gentamicin with minocycline as catheter lock solutions in the prevention of catheter-related bacteremia. Am J Kidney Dis. 2006;48(4):596–605. [PubMed: 16997056]
Peterson WJ, Maya ID, Carlton D et al. Treatment of dialysis catheter-related Enterococcus bacteremia with an antibiotic lock: a quality improvement report. American journal of kidney diseases. 2009;53:107–111.
Poole CV, Carlton D, Bimbo L et al. Treatment of catheter-related bacteraemia with an antibiotic lock protocol: effect of bacterial pathogen. Nephrology Dialysis Transplantation. 2004;19:1237–1244.
Rabindranath KS, Bansal T, Adams J et al. Systematic review of antimicrobials for the prevention of haemodialysis catheter-related infections. Nephrology Dialysis Transplantation. 2009;24:3763–3774.
Rackoff WR, Weiman M, Jakobowski D, et al. A randomized, controlled trial of the efficacy of a heparin and vancomycin solution in preventing central venous catheter infections in children. J Pediatr. 1995;127(1):147–151. [PubMed: 7608801].
Saad TF. Bacteremia associated with tunneled, cuffed hemodialysis catheters. American journal of kidney diseases. 1999;34:1114–1124.
Safdar N, Maki DG. Use of vancomycin-containing lock or flush solutions for prevention of bloodstream infection associated with central venous access devices: a meta-analysis of prospective, randomized trials. Clin Infect Dis 2006;43:474–484.
Saxena AK, Panhotra BR, Sundaram DS, et al. Tunneled catheters' outcome optimization among diabetics on dialysis through antibiotic-lock placement. Kidney Int. 2006;70(9):1629–1635. [PubMed: 16955110].
Saxena AK, Panhotra BR, Sundaram DS, Naguib M, Morsy F, Al-Ghamdi AMA. Enhancing the survival of tunneled hemodialysis catheters using an antibiotic lock in the elderly: a randomised, double-blind clinical trial. Nephrology. 2006;11(4):99–305.
Saxena AK, Panhotra BR. The impact of catheter-restricted filling with cefotaxime and heparin on the lifespan of temporary hemodialysis catheters: a case controlled study. J Nephrol 2005;18:755–763.
Schwartz C, Henrickson KJ, Roghmann K, Powell K. Prevention of bacteremia attributed to luminal colonization of tunneled central venous catheters with vancomycin-susceptible organisms. J Clin Oncol. 1990;8(9):1591–1597. [PubMed: 2202792].
Snaterse M, Ruger W, Scholte OP et al. Antibiotic-based catheter lock solutions for prevention of catheter-related bloodstream infection: a systematic review of randomised controlled trials. J Hosp Infect 2010;75:1–11.
Snaterse M, Rüger W, Scholte Op Reimer WJ, Lucas C. Antibiotic-based catheter lock solutions for prevention of catheter-related bloodstream infection: a systematic review of randomised controlled trials. J Hosp Infect. 2010 May;75(1):1–11. Doi: 10.1016/j.jhin.2009.12.017. Epub 2010 Mar 15.
Solomon LR, A randomized double-blind controlled trial of taurolidine-citrate catheter locks for the prevention of bacteremia in patients treated with hemodialysis. Am J KidneyDis 2010;55:1060–1068.
Tejwani RMD and Parry MFMD. Antimicrobial Lock Therapy as an Adjunct to Management of Catheter-Related Bacteremia: A Community Hospital Experience. Infectious Diseases in Clinical Practice. 2011;19:256–261.
Winnicki W, Herkner H, Lorenz M, Handisurya A, Kikić Ž, Bielesz B, Schairer B, Reiter T, Eskandary F, Sunder-Plassmann G, Sengoelge G. Taurolidine-based catheter lock regimen significantly reduces overall costs, infection, and dysfunction rates of tunneled hemodialysis catheters. Kidney Int. 2018 Mar;93(3):753–760. Doi: 10.1016/j.kint.2017.06.026. Epub 2017 Sep 8.
Yahav D, Rozen-Zvi B, Gafter-Gvili A, Leibovici L, Gafter U, Paul M. Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients undergoing hemodialysis: systematic review and meta-analysis of randomized, controlled trials. Clin Infect Dis. 2008 Jul 1;47(1):83–93. Doi: 10.1086/588667.
6.4. Предлагаем не использовать профилактический антибактериальный раствор для внутрипросветной экспозиции у взрослых пациентов при состояниях при ОПП нетуннелированными центральными венозными катетерами для гемодиализа для профилактики катетер-ассоциированной инфекции кровотока.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
O’Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Infect Control Hosp Epidemiol 2002;23:759–769.
Marschall J, Mermel LA, Classen D, et al. Strategies to prevent central lineassociated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol 2008;29(Suppl 1):S22–30.
Pratt RJ, Pellowe CM, Wilson JA, et al. epic2: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. J Hosp Infect 2007;65(Suppl 1):S1–64.
6.5. Предлагаем корректировать дисфункцию туннелированного катетера для гемодиализа или восстановить его проходимость введением фибринолитических средств в просвет катетера до обмена по проводнику или изменения места локализации у взрослых пациентов при состояниях при ХБП-5.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Дисфункция катетера может быть сведена к минимуму при использовании отвечающего современным требованиям материала, из которого сделан катетер, идеальной техники введения и при неукоснительном выполнении протоколов по уходу за катетером. Повторная дисфункция катетера для гемодиализа требует повторного введения в просвет фибринолитических средств, визуализацию дистального сегмента катетера, микробиологического обследования и оценку системный коагуляции у взрослых пациентов при состояниях при ХБП-5.
Allon M, Brouwer-Maier DJ, Abreo K, Baskin KM, Bregel K, Chand DH, Easom AM, Mermel L, Mokrzycki MH, Patel P R, Roy-Chaudhur P, Shenoy S, Valentini RP, Wasse H Recommended Clinical Trial End Points for Dialysis Catheters. Clin J Am Soc Nephrol. 2018 Mar 7;13(3):495–500. Doi: 10.2215/CJN.12011116. Epub 2017 Jul 20.
Clase CM, Crowther MA, Ingram AJ, Cina CS. Thrombolysis for restoration of patency to haemodialysis central venous catheters: a systematic review. J Thromb Thrombolysis 2001;11:127–136.
Gray RJ, Levitin A, Buck D, Brown LC, Sparling YH, Jablonski KA, Fessahaye A, Gupta AK. Percutaneous fibrin sheath stripping versus transcatheter urokinase infusion for malfunctioning well-positioned tunneled central venous dialysis catheters: a prospective, randomized trial. J Vasc Interv Radiol. 2000 Oct;11(9):1121–1129.
Hemmelgarn BR, Moist LM, Lok CE, TonelliM, Manns BJ,Holden RM, LeBlanc M, Faris P, Barre P, Zhang J, Scott-Douglas N; Prevention of Dialysis Catheter Lumen Occlusion with rt-PA versus Heparin Study Group: Prevention of dialysis catheter malfunction with recombinant tissue plasminogen activator.NEngl J Me 364:303–312, 2011.
Little MA, Walshe JJ. A longitudinal study of the repeated use of alteplase as therapy for tunneled hemodialysis catheter dysfunction. Am J Kidney Dis. 2002 Jan;39(1):86–91.
Merport M, Murphy TP, Egglin TK, Dubel GJ. Fibrin sheath stripping versus catheter exchange for the treatment of failed tunneled hemodialysis catheters: randomized clinical trial. J Vasc Interv Radiol 2000;11:1115–1120.
Mokrzycki MH, Jean-Jerome K, Rush H, Zdunek MP, Rosenberg SO. A randomized trial of minidose warfarin for the prevention of late malfunction in tunneled, cuffed hemodialysis catheters. Kidney Int 2001;59:1935–1942.
Oliver MJ, Mendelssohn DC, Quinn RR, Richardson EP, Rajan DK, Pugash RA, Hiller JA, Kiss AJ, Lok CE. Catheter patency and function after catheter sheath disruption: a pilot study. Clin J Am Soc Nephrol. 2007 Nov;2(6):1201–1206. Epub 2007 Oct 17.
Tumlin J, Goldman J, Spiegel DM, Roer D, Ntoso KA, Blaney M, Jacobs J, Gillespie BS, Begelman SM. A phase III, randomized, double-blind, placebo-controlled study of tenecteplase for improvement of hemodialysis catheter function: TROPICS 3. Clin J Am Soc Nephrol. 2010 Apr;5(4):631–636. Doi: 10.2215/CJN.06520909. Epub 2010 Feb 4.
Yaseen O, El-Masri MM, El Nekidy WS et al. Comparison of alteplase (tissue plasminogen activator) high-dose vs. low-dose protocol in restoring hemodialysis catheter function: The ALTEDOSE study. Hemodial. Int. 2013;17:434–440.
Zacharias JM, Weatherston CP, Spewak CR, Vercaigne LM. Alteplase versus urokinase for occluded hemodialysis catheters. Ann Pharmacother 2003;37:27–33.
7. Удаление катетера для диализа
7.1. Рекомендуем удалить центральный венозный катетер для гемодиализа незамедлительно – как только необходимость в нем отпала.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Нетуннелированный катетер должен быть удален как можно скорее, чтобы уменьшить риск инфекционных осложнений, или при необходимости обменен на туннелированный катетер, когда станет ясно, что восстановление почек маловероятно в ближайшей перспективе. Туннелированные катетеры для гемодиализа часто удаляются так же легко, как нетуннелированные, в течение первых недель после имплантации, но их удаление обычно более инвазивно и требует тем больше времени, чем дольше они стоят.
Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32(10):2014–2020. [PubMed: 15483409].
Cook D, Randolph A, Kernerman P, et al. Central venous catheter replacement strategies: a systematic review of the literature. Crit Care Med 1997;25(8):1417–1424.
Gillies D,Wallen MM, Morrison AL, Rankin K, Nagy SA, O’Riordan E. Optimal timing for intravenous administration set replacement. Cochrane Database of Systematic Reviews. 2005; Issue 4. Art. No.:CD003588. Doi: 10.1002/14651858.CD003588.pub2.
Lederle FA, Parenti CM, Berskow LC, Ellingson KJ. The idle intravenous catheter. Ann Intern Med. 1992;116(9):737–738. [PubMed: 1558345].
Parenti CM, Lederle FA, Impola CL, Peterson LR. Reduction of unnecessary intravenous catheter use Internal medicine house staff participate in a successful quality improvement project. Arch Intern Med. 1994;154(16):1829–1832.[PubMed: 8053750].
Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–2732. [PubMed: 17192537]
Saleh HM, Abouellail H. Prospective, randomized study of tunneled cuffed hemodialysis catheter removal and delayed insertion, versus guidewire exchange to treat catheter related blood stream infection. Interim results of first 100 cases. Life Sci J 2017;14:45–49.
Saleh HM, Tawfik MM, Abouellail H. Prospective, randomized study of long-term hemodialysis catheter removal versus guidewire exchange to treat catheter-related bloodstream infection. J Vasc Surg. 2017;66(5):1427–1431. e1421.
7.2. Рекомендуем незамедлительно удалять нетуннелированный катетер для гемодиализа при появлении местных и/или системных признаков воспаления, в отсутствие альтернативных источников инфекции.
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Удаление катетера для гемодиализа следует считать первым шагом в лечении. Отказ от нетуннелированного катетера должен быть немедленным, когда инфекция диагностирована. Если нетуннелированный катетер сместился наружу, не следует проталкивать его внутрь. Необходимо установить, располагается ли он в сосудистом русле, если да, то застабилизировать в этом положении и только затем проводить дальнейшие манипуляции. В иных случаях нетуннелированный катетер немедленно удалить.
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis 2004;44(5):779–791.
Cook D, Randolph A, Kernerman P, et al. Central venous catheter replacement strategies: a systematic review of the literature. Crit Care Med 1997;25(8):1417–1424.
Gillies D,Wallen MM, Morrison AL, Rankin K, Nagy SA, O’Riordan E. Optimal timing for intravenous administration set replacement. Cochrane Database of Systematic Reviews. 2005;Issue 4. Art. No.:CD003588. Doi: 10.1002/14651858.CD003588.pub2.
Marr KA, Sexton DI, Conlon PJ, Corey et al. Catheter related bacteraemia and outcome of attempted catheter salvage in patients undergoing hemodialysis. Ann Intern Med 1997;127:275–280.
Saleh HM, Tawfik MM, Abouellail H. Prospective, randomized study of long-term hemodialysis catheter removal versus guidewire exchange to treat catheter-related bloodstream infection. J Vasc Surg. 2017;66(5):1427–1431. e1421.
7.3. Рекомендуем считать первым необходимым шагом в лечении – это удаление туннелированного катетера для гемодиализа при лихорадке или бактериемии более 48–72 часов от начала лечения, при специфических вирулентных микроорганизмах или менее вирулентных, но трудноподдающихся лечению (S. aureus, P. aeruginosa, Pseudomonas spp., Candida spp., микобактерии, мультирезистентные микроорганизмы, полирезистентная инфекция), при тяжелых осложнениях (туннельная инфекция, сепсис и метастатическая инфекция).
Уровень достоверности доказательств I, уровень убедительности рекомендаций A
Комментарии. Не удаляйте туннелированный катетер для гемодиализа только на основании лихорадки. Используйте клиническое мышление относительно целесообразности удаления катетера, если доказана инфекция в другом месте или если подозревается неинфекционная причина лихорадки. Удаление должно быть сбалансировано с потенциальными вариантами будущего альтернативного доступа для диализа взрослых пациентов при состояниях при ХБП-5.
Aslam S, Vaida F, Ritter M, Mehta RL. Systematic review and metaanalysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol: JASN. 2014;25(12):2927–2941.
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis 2004;44(5):779–791.
Ashby DR, Power A, Singh S, Choi P, Taube DH, Duncan ND, Cairns TD Bacteremia associated with tunneled hemodialysis catheters: outcome after attempted salvage. Clin J Am Soc Nephrol. 2009 Oct;4(10):1601–1605. Doi: 10.2215/CJN.01840309. Epub 2009 Aug 13.
Almasri J, Alsawas M, Mainou M, et al. Outcomes of vascular access for hemodialysis: a systematic review and meta-analysis. J Vasc Surg. 2016;64(1):236–243.
Beathard GA, Urbanes A Infection associated with tunneled hemodialysis catheters. Semin Dial. 2008 Nov–Dec;21(6):528–538. Doi: 10.1111/j.1525-139X.2008.00497.x. Epub 2008 Sep 24.
Garnacho-Montero J, Aldabo-Pall as T, Palomar-Martınez M, et al. Risk factors and prognosis of catheter-related bloodstream infection in critically ill patients: a multicenter study. Intensive Care Med. 2008;34:2185–2193.
Marr KA, Sexton DI, Conlon PJ, Corey et al. Catheter related bacteraemia and outcome of attempted catheter salvage in patients undergoing hemodialysis. Ann Intern Med 1997;127:275–280.
Maki DG, Kluger DM, Crnich CJ. The risk of bloodstream infection in adults with different intravascular devices: a systematic review of 200 published prospective studies. Mayo Clinic proceedings Mayo Clinic. 2006;81(9):1159–1171. [PubMed: 16970212].
Lemaire X, Morena M, Leray-Moragues H et al. Analysis of risk factors for catheter-related bacteremia in 2000 permanent dual catheters for hemodialysis. Blood Purif 2009; 8:21–28.
Tomlinson D, Mermel LA, Ethier MC, Matlow A, Gillmeister B, Sung L. Defining bloodstream infections related to central venous catheters in patients with cancer: a systematic review. Clin Infect Dis 2011;53(7):697–710.
Rosenthal VD. Central Line-Associated Bloodstream Infections in Limited-Resource Countries: A Review of the Literature. Clin Infect Dis. 2009;49:1899–1907. Doi: 10.1086/648439.
Renaud B, Brun-Buisson C. Outcomes of primary and catheter-related bacteremia A cohort and case-control study in critically ill patients. Am J Respir Crit Care Med. 2001; 163(7):1584–1590. [PubMed: 11401878]
Ravani P, Palmer SC, Oliver MJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol: JASN. 2013;24(3):465–473.
Saleh HM, Abouellail H. Prospective, randomized study of tunneled cuffed hemodialysis catheter removal and delayed insertion, versus guidewire exchange to treat catheter related blood stream infection. Interim results of first 100 cases. Life Sci J. 2017;14:45–49.
7.4. Предлагаем извлеченный катетер (дистальный конец) для гемодиализа направлять на микробиологическое исследование вместе с пробами крови из экстракорпорального контура или периферических вен.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Boyd A, Dunne A, Townsend K, Pai AB.Sampling for international normalized ratios in patients on hemodialysis with central venous catheters. Nephrol Nurs J. 2006 Jul–Aug;33(4):408–411.
7.5. Рекомендуем считать необходимым удаление катетер для гемодиализа с его последующим введением в иной анатомической локализации при наличии признаков инфицирования места выхода катетера и/или признаков системной воспалительной реакции без четкой связи с наличием локальной инфекции.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. При необходимости поддержания сосудистого доступа ЦВК переустанавливают в другой анатомической области. Не следует переустанавливать ЦВК по проводнику. Инфекция места выхода туннельного катетера должна лечиться подходящими антибиотиками в течение 2 недель (4 недели при наличии бактериемии).
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis. 2004;44:779.
Almasri J, Alsawas M, Mainou M, et al. Outcomes of vascular access for hemodialysis: a systematic review and meta-analysis. J Vasc Surg. 2016;64(1):236–243.
Aslam S, Vaida F, Ritter M, Mehta RL Systematic review and meta-analysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol. 2014 Dec;25(12):2927–2941. Doi: 10.1681/ASN.2013091009. Epub 2014 May 22.
Cook D, Randolph A, Kernerman P, et al. Central venous catheter replacement strategies: a systematic review of the literature. Crit Care Med 1997;25(8):1417–1424.
Gillies D, Wallen MM, Morrison AL, Rankin K, Nagy SA, O’Riordan E. Optimal timing for intravenous administration set replacement. Cochrane Database of Systematic Reviews. 2005; Issue 4. Art. No.: CD003588. Doi: 10.1002/14651858.CD003588.pub2.
Maya ID. Antibiotic lock for treatment of tunneled hemodialysis catheter bacteremia. Semin Dial. 2008;21:539–541.
Ravani P, Palmer SC, Oliver MJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol: JASN. 2013;24(3):465–473.
Saleh HM, Abouellail H. Prospective, randomized study of tunneled cuffed hemodialysis catheter removal and delayed insertion, versus guidewire exchange to treat catheter related blood stream infection. Interim results of first 100 cases. Life Sci J. 2017;14:45–49.
Saleh HM, Tawfik MM, Abouellail H. Prospective, randomized study of long-term hemodialysis catheter removal versus guidewire exchange to treat catheter-related bloodstream infection. J Vasc Surg. 2017;66(5):1427–1431. e1421.
Vats HS: Complications of catheters: Tunneled and non tunneled. Adv Chronic Kidney Dis 19:188–194, 2012.
Willicombe MK, Vernon K, Davenport A Embolic complications from central venous hemodialysis catheters used with hypertonic citrate locking solution. Am J Kidney Dis. 2010 Feb;55(2):348–351. Doi: 10.1053/j.ajkd.2009.06.037. Epub 2009 Oct 2.
7.6. Предлагаем рассматривать отсроченное удаление туннелированного катетера для гемодиализа при наличии непродолжительной фебрильной температуры и/или проявлений бактериемии.
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
Комментарии. Удаление может быть отложено на несколько дней при использовании туннелированных катетеров. Если отсутствует информация о возбудителе, эмпирическая антимикробная терапия должна быть назначена. Этот консервативный вариант подразумевает, что пациент регулярно и тщательно все соблюдает, внутрипросветная кспозиция раствора с антибиотиком назначается после каждой процедуры, назначается адекватная парентеральная антибактериальная терапия на 2 недели. Риск септических осложнений отсроченного удаления катетера должен быть сбалансирован с преимуществами сохранения доступа для диализа.
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis. 2004;44:779.
Allon M. Prophylaxis against dialysis catheter-related bacteremia with a novel antimicrobial lock solution. Clin Infect Dis. 2003; 36(12):1539–1544. [PubMed: 12802753].
Allon M. Treatment guidelines for dialysis catheter-related bacteremia – an update. Am J Kidney Dis. 2009;54:13–17.
Ashby DR, Power A, Singh S, Choi P, Taube DH, Duncan ND, Cairns TD Bacteremia associated with tunneled hemodialysis catheters: outcome after attempted salvage. Clin J Am Soc Nephrol. 2009 Oct;4(10):1601–1605. Doi: 10.2215/CJN.01840309. Epub 2009 Aug 13.
Beathard GA. Management of bacteremia associated with tunneled-cuffed hemodialysis catheters. Journal of the American Society of Nephrology. 1999;10:1045–1049.
Bleyer AJ, Mason L, Russell G, Raad II, Sherertz RJ. A randomized, controlled trial of a new vascular catheter flush solution (minocycline-EDTA) in temporary hemodialysis access. Infect Control Hosp Epidemiol. 2005;26(6):520–524. [PubMed: 16018426]
Donlan RM Biofilm formation: a clinically relevant microbiological process. Clin Infect Dis. 2001 Oct 15;33(8):1387–1392. Epub 2001 Sep 20.
Fernandez-Hidalgo N, Almirante B, Calleja R, Ruiz I, Planes AM, Rodriguez D, Pigrau C, Pahissa A. Antibiotic-lock therapy for long-term intravascular catheter-related bacteraemia: results of an open, non-comparative study. J Antimicrob Chemother. 2006 Jun;57(6):1172–1180. Epub 2006 Apr 5.
Fortún J, Grill F, Martín-Dávila P, Blázquez J, Tato M, Sánchez-Corral J, García-San Miguel L, Moreno S Treatment of long-term intravascular catheter-related bacteraemia with antibiotic-lock therapy. J Antimicrob Chemother. 2006 Oct;58(4):816–821. Epub 2006 Aug 8.
Grudzinski L, Quinan P, Kwok S, Pierratos A. Sodium citrate 4% locking solution for central venous dialysis catheters – an effective, more cost-efficient alternative to heparin. Nephrol Dial Transplant. 2007 Feb;22(2):471–476. Epub 2006 Oct 25.
Kim SH, Song KI, Chang JW, et al. Prevention of uncuffed hemodialysis catheter-related bacteremia using an antibiotic lock technique: a prospective, randomized clinical trial. Kidney Int. 2006;69(1):161–164. [PubMed: 16374438].
Krishnasami Z, Carlton D, Bimbo L, Taylor ME, Balkovetz DF, Barker J, Allon M. Management of hemodialysis catheter-related bacteremia with an adjunctive antibiotic lock solution. Kidney Int. 2002 Mar;61(3):1136–1142.
Labriola L, Crott R, and Jadoul M. Preventing haemodialysis catheter-related bacteraemia with an antimicrobial lock solution: a meta-analysis of prospective randomized trials. Nephrology Dialysis Transplantation. 2008;23:1666–1672.
Labriola L. Antibiotic locks for the treatment of catheter‐related blood stream infection: Still more hope than data Semm Dial 2019 Apr 4. Doi: 10.111 1/sdi. 12807 [Epub ahead of print].
Lok CE, Appleton D, Bhola C, Khoo B, Richardson RM.Trisodium citrate 4% – an alternative to heparin capping of haemodialysis catheters. Nephrol Dial Transplant. 2007 Feb;22(2):477–483. Epub 2006 Oct 2.
Lomas Cabezas JM, Luque Marquez R, Documento de consenso sobre infecciones relaconadas vascuiares V 12 suplemento 1, 2011.
Maya ID, Carlton D, Estrada E, Allon M. Treatment of dialysis catheter-related Staphylococcus aureus bacteremia with an antibiotic lock: a quality improvement report. Am J Kidney Dis. 2007 Aug;50(2):289–295.
McIntyre CW, Hulme LJ, Taal M, Fluck RJ. Locking of tunneled hemodialysis catheters with gentamicin and heparin. Kidney Int. 2004;66:801–805.
Mermel LA What is the evidence for intraluminal colonization of hemodialysis catheters? Kidney Int. 2014 Jul;86(1):28–33. Doi: 10.1038/ki.2013.527. Epub 2014 Jan 8.
Mermel LA1 .Prevention of intravascular catheter infections--insights and prospects for hemodialysis catheters. Nephrologie. 2001;22(8):449–451.
Mokrzycki MH1, Zhang M, Cohen H, Golestaneh L, Laut JM, Rosenberg SO.Tunnelled haemodialysis catheter bacteraemia: risk factors for bacteraemia recurrence, infectious complications and mortality. Nephrol Dial Transplant. 2006 Apr;21(4):1024–1031. Epub 2006 Jan 31.
Nori US, Manoharan A, Yee J, Besarab A. Comparison of low-dose gentamicin with minocycline as catheter lock solutions in the prevention of catheter-related bacteremia. Am J Kidney Dis. 2006;48(4):596–605. [PubMed: 16997056].
Onder AM, Chandar J, Billings AA, Simon N, Diaz R, Francoeur D, Abitbol C, Zilleruelo G.Comparison of early versus late use of antibiotic locks in the treatment of catheter-related bacteremia. Clin J Am Soc Nephrol. 2008 Jul;3(4):1048–1056. Doi: 10.2215/CJN.04931107. Epub 2008 Apr 9.
Peterson WJ, Maya ID, Carlton D et al. Treatment of dialysis catheter-related Enterococcus bacteremia with an antibiotic lock: a quality improvement report. American journal of kidney diseases. 2009;53:107–111.
Poole CV, Carlton D, Bimbo L et al. Treatment of catheter-related bacteraemia with an antibiotic lock protocol: effect of bacterial pathogen. Nephrology Dialysis Transplantation. 2004;19:1237–1244.
Raad I, Hanna H, Maki D. Intravascular catheter-related infections: advances in diagnosis, prevention, and management.Lancet Infect Dis. 2007 Oct;7(10):645–657. Review.
Robinson D, Suhocki P, Schwab SJ. Treatment of infected tunneled venous access hemodialysis catheters with guidewire exchange. Kidney Int. 1998 Jun;53(6):1792–1794.
Saad TF. Bacteremia associated with tunneled, cuffed hemodialysis catheters. American journal of kidney diseases. 1999;34:1114–1124.
Saxena AK, Panhotra BR, Sundaram DS, et al. Tunneled catheters' outcome optimization among diabetics on dialysis through antibiotic-lock placement. Kidney Int. 2006;70(9):1629–1635. [PubMed: 16955110].
Shaffer D. Catheter-related sepsis complicating long-term, tunnelled central venous dialysis catheters: management by guidewire exchange. Am J Kidney Dis. 1995 Apr;25(4):593–596.
Tanriover B, Carlton D, Saddekni S et al. Bacteraemia associated with tunneled dialysis catheters: camparison of two treatment strategies. Kidney Int 2000;5:2151–2155.
Vardhan A, Davies J, Daryanani I, Crowe A, McClelland P. Treatment of haemodialysis catheter-related infections. Nephrol Dial Transplant. 2002 Jun;17(6):1149–1150.
Weijmer MC, van den Dorpel MA, Van de Ven PJ et al. Randomised clinical trial comparison of trisodium citrate 30% and heparin as catheter-locking solution in haemodialysis patients. J Am Soc Nephrol 2005;16:2769–2777.
8. Обмен катетера для диализа
8.1. Предлагаем не обменивать рутинно нетуннелированные катетеры для гемодиализа с целью предотвращения инфекций кровотока.
Уровень достоверности доказательств II, уровень убедительности рекомендаций B
Eyer S, Brummitt C, Crossley K, Siegel R, Cerra F.Catheter-related sepsis: prospective, randomized study of three methods of long-term catheter maintenance. Crit Care Med. 1990 Oct;18(10):1073–1079.
Cook D, Randolph A, Kernerman P, Cupido C, King D, Soukup C, Brun-Buisson C.Central venous catheter replacement strategies: a systematic review of the literature.Crit Care Med. 1997 Aug;25(8):1417–1424. Review.
Cobb DK, High KP, Sawyer RG, Sable CA, Adams RB, Lindley DA, Pruett TL, Schwenzer KJ, Farr BM. A controlled trial of scheduled replacement of central venous and pulmonary-artery catheters. N Engl J Med. 1992 Oct 8;327(15):1062–1068.
8.2. Рекомендуем не использовать проводник для обмена при наличии подозрений на инфекцию нетуннелированного катетера для гемодиализа.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Комментарии. Используйте проводник для замены нефункционирующего нетуннелированного катетера, если нет доказательств его инфицирования.
Aslam S, Vaida F, Ritter M, Mehta RL.Systematic review and meta-analysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol. 2014 Dec;25(12):2927–2941. Doi: 10.1681/ASN.2013091009. Epub 2014. May 22.
Bonawitz SC, Hammell EJ, Kirkpatrick JR. Prevention of central venous catheter sepsis: a prospective randomized trial. Am Surg. 1991 Oct;57(10):618–623.
Cobb DK, High KP, Sawyer RG, Sable CA, Adams RB, Lindley DA, Pruett TL, Schwenzer KJ, Farr BM. A controlled trial of scheduled replacement of central venous and pulmonary-artery catheters. N Engl J Med. 1992 Oct 8;327(15):1062–1068.
Cook D, Randolph A, Kernerman P, Cupido C, King D, Soukup C, Brun-Buisson C.Central venous catheter replacement strategies: a systematic review of the literature.Crit Care Med. 1997 Aug;25(8):1417–1424. Review.
Eyer S, Brummitt C, Crossley K, Siegel R, Cerra F.Catheter-related sepsis: prospective, randomized study of three methods of long-term catheter maintenance. Crit Care Med. 1990 Oct;18(10):1073–1079.
Saleh HM, Tawfik MM, Abouellail H. Prospective, randomized study of long-term hemodialysis catheter removal versus guidewire exchange to treat catheter-related bloodstream infection. J Vasc Surg. 2017 Nov;66(5):1427–1431.e1. Doi: 10.1016/j.jvs.2017.05.119. Epub 2017 Aug 16.
Tanriover B, Carlton D, Saddekni S et al. Bacteraemia associated with tunneled dialysis catheters: camparison of two treatment strategies. Kidney Int 2000;5:2151-5
8.3. Для спасения и сохранения сосудистого доступа предлагаем обменивать туннелированные катетеры для гемодиализа по проводнику взрослым пациентам при состояниях при ХБП-5, при ограниченном количестве мест доступа для диализа.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Комментарии. Обмен ЦВК по проводнику является безопасным, эффективным и жизнеспособным вариантом с точки зрения выживания катетера как доступа для диализа и внутрибольничной инфекции. Обмен по проводнику связан со значительно большей безрецидивной выживаемостью катетера, чем при ранней и поздней внутрипросветной экспозиции раствором с антибиотиком.
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis. 2004;44:779.
Ashby DR, Power A, Singh S, Choi P, Taube DH, Duncan ND, Cairns TD Bacteremia associated with tunneled hemodialysis catheters: outcome after attempted salvage. Clin J Am Soc Nephrol. 2009 Oct;4(10):1601–1605. Doi: 10.2215/CJN.01840309. Epub 2009 Aug 13.
Beathard GA. Urbanes AInfection associated with tunneled hemodialysis catheters. Semin Dial. 2008 Nov-Dec;21(6):528–538. Doi: 10.1111/j.1525-139X.2008.00497.x. Epub 2008 Sep 24.
Casey J, Davies J, Balshaw-Greer A et al. Inserting tunnelled hemodialysis catheters using elective guidewire exchange from nontunnelled catheters: is there a greater risk of infection when compared with new-site replacement? Hemodialysis International. 2008;12:52–54.
Falk A, Parthasarathy S. Conversion of temporary hemodialysis catheters to tunneled hemodialysis catheters. Clinical Nephrology. 2005;63:209–214.
Garnacho-Montero J, Aldabo-Pall as T, Palomar-Martınez M, et al. Risk factors and prognosis of catheter-related bloodstream infection in critically ill patients: a multicenter study. Intensive Care Med. 2008;34:2185–2193.
Hou S-M, Chou P-C, Huang C-H et al. Is guidewire exchange a better approach for subclavian vein re-catheterization for chronic hemodialysis patients? Thrombosis Research. 2006;118:439–445.
Marr KA, Sexton DJ, Conlon PJ, Corey GR, Schwab SJ, Kirkland KB.Catheter-related bacteremia and outcome of attempted catheter salvage in patients undergoing hemodialysis. Ann Intern Med. 1997 Aug 15;127(4):275–280.
Powell S, Chan TY, Bhat R et al. A retrospective comparative study of tunneled haemodialysis catheters inserted through occluded or collateral veins versus conventional methods. Cardiovascular & Interventional Radiology. 2010;33:744–750.
Saleh HM, Tawfik MM, Abouellail H .Prospective, randomized study of long-term hemodialysis catheter removal versus guidewire exchange to treat catheter-related bloodstream infection. J Vasc Surg. 2017 Nov;66(5):1427–1431. e1. Doi: 10.1016/j.jvs.2017.05.119. Epub 2017 Aug 16.
Shaffer D. Catheter-related sepsis complicating long-term, tunnelled central venous dialysis catheters: management by guidewire exchange. Am J Kidney Dis. 1995 Apr;25(4):593–596.
Tanriover B, Carlton D, Saddekni S et al. Bacteraemia associated with tunneled dialysis catheters: camparison of two treatment strategies. Kidney Int 2000;5:2151–2155.
Taylor G, Gravel D, Johnston L et al. Incidence of bloodstream infection in multicenter inception cohorts of hemodialysis patients. American journal of infection control. 2004;32:155–160.
8.4. Предлагаем взрослым пациентам при неосложненной бактериемии с положительными результатами в посевах крови при состояниях при ХБП-5 обменивать туннелированные катетеры по проводнику, если лихорадка разрешилась и симптомы быстро исчезли через 48–72 часа после начала эффективного лечения, при этом пациент остается клинически стабильным и отсутствуют признаки туннельной инфекции.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Комментарии. Нет необходимости регулярно подтверждать отрицательные результаты после обмена катетера, если у пациента нет симптомов (т.е. отсутствие лихорадки или озноба).
Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis. 2004;44:779.
Aslam S, Vaida F, Ritter M, Mehta RL.Systematic review and meta-analysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol. 2014 Dec;25(12):2927–2941. Doi: 10.1681/ASN.2013091009. Epub 2014. May 22.
Beathard GA. Management of bacteremia associated with tunneled-cuffed hemodialysis catheters. Journal of the American Society of Nephrology. 1999;10:1045–1049.
Krishnasami Z, Carlton D, Bimbo L, Taylor ME, Balkovetz DF, Barker J, Allon M. Management of hemodialysis catheter-related bacteremia with an adjunctive antibiotic lock solution. Kidney Int. 2002 Mar;61(3):1136–1142.
Labriola L. Antibiotic locks for the treatment of catheter‐related blood stream infection: Still more hope than data Semm Dial 2019 Apr 4. Doi: 10.111 1/sdi. 12807 [Epub ahead of print].
Mermel LA, Allon M, Bouza E et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009. Update by the Infectious Diseases Society of America. Clinical infectious diseases. 2009;49:1–45.
Mokrzycki MH, Zhang M, Cohen H, Golestaneh L, Laut JM, Rosenberg SOTunnelled haemodialysis catheter bacteraemia: risk factors for bacteraemia recurrence, infectious complications and mortality. Nephrol Dial Transplant. 2006 Apr;21(4):1024–1031. Epub 2006 Jan 31.
Onder AM, Chandar J, Billings AA, Simon N, Diaz R, Francoeur D, Abitbol C, Zilleruelo G. Comparison of early versus late use of antibiotic locks in the treatment of catheter-related bacteremia. Clin J Am Soc Nephrol. 2008 Jul;3(4):1048–1056. Doi: 10.2215/CJN.04931107. Epub 2008 Apr 9.
Saleh HM, Tawfik MM, Abouellail H. Prospective, randomized study of long-term hemodialysis catheter removal versus guidewire exchange to treat catheter-related bloodstream infection. J Vasc Surg. 2017 Nov;66(5):1427–1431. e1. Doi: 10.1016/j.jvs.2017.05.119. Epub 2017 Aug 16.
Sychev D, Maya ID, Allon M. Clinical outcomes of dialysis catheter-related candidemia in hemodialysis patients. Clin J Am Soc Nephrol. 2009 Jun;4(6):1102–1105. Doi: 10.2215/CJN.01610309. Epub 2009 Apr 30.
Tanriover B, Carlton D, Saddekni S et al. Bacteraemia associated with tunneled dialysis catheters: camparison of two treatment strategies. Kidney Int 2000;5:2151–2155.
ДОСТУП ДЛЯ ПЕРИТОНЕАЛЬНОГО ДИАЛИЗА
1.1. Катетеры, используемые взрослыми пациентами при состояниях при ХБП-5, которым показана медицинская помощь методами перитонеального диализа.
1.2. Рекомендуем катетеры для перитонеального диализа, изготовленные из силиконовой резины.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Crabtree JH. Clinical biodurability of aliphatic polyether-based polyurethanes as peritoneal dialysis catheters. ASAIO J 2003;49:290–294.
Gardezi AI, Schlageter KW, Foster DM, Astor BC, Chan MR, Waheed S. Erosion of the silicone peritoneal dialysis catheter with the use of gentamicin cream at the exit site. Adv Perit Int 2016;32:15–18.
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor. Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi: 10.3747/pdi.2018.00232.
1.3. Рекомендуем стандартные катетеры для перитонеального диализа, снабженные устройством для фиксации катетера, двойными манжетами из дакрона (полиэфира).
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Eklund B, Honkanen E, Kyllonen L, Salmela K, Kala AR. Peritoneal dialysis access: prospective randomized comparison of single-cuff and double-cuff straight Tenckhoff catheters. Nephrol Dial Transplant 1997; 12:2664–2666.
Nessim SJ, Bargman JM, Jassal SV. Relationship between double-cuff versus single-cuff peritoneal dialysis catheters and risk of peritonitis. Nephrol Dial Transplant 2010; 25:2310–2334.
Vychytil A, Lorenz M, Schneider B, Hörl WH, Haag-Weber M. New strategies to prevent Staphylococcus aureus infections in peritoneal dialysis patients. J Am Soc Nephrol 1998; 9:669–676.
1.4. Рекомендуем в равной степени использовать катетеры для перитонеального диализа с прямым или спирально закрученным дистальным сегментом катетера, в равной степени прямые или предварительно сформированные угловым изгибом в сегменте между манжетами.
Уровень достоверности доказательств I, уровень убедительности рекомендаций C
Hagen SM, Lafranca JA, IJzermans JN, Dor FJ. A systematic review and meta-analysis of the influence of peritoneal dialysis catheter type on complication rate and catheter survival. Kidney Int 2014;85:920–932.
Xie J, Kiryluk K, Ren H, Zhu P, Huang X, Shen P, et al. Coiled versus straight peritoneal dialysis catheters: a randomized controlled trial and meta-analysis. Am J Kidney Dis 2011;58:946–955.
1.5. При удаленном расположении места выхода катетера от места его дистальной локации рекомендуем использовать удлиненный катетер для перитонеального диализа, когда стандартные катетеры не могут обеспечить оптимальное положение дистального сегмента катетера в тазу и соответствующее требованиям место выхода катетера.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Crabtree JH, Burchette RJ. Comparative analysis of two-piece extended peritoneal dialysis catheters with remote exit-site locations and conventional abdominal catheters. Perit Dial Int 2010;30:46–55.
Crabtree JH. Extended peritoneal dialysis catheters for upper abdominal wall exit sites. Perit Dial Int 2004;24:292–294.
Eriguchi M, Tsuruya K, Yoshida H, Haruyama N, Tanaka S, Tsuchimoto A, et al. Extended swan-neck catheter with upper abdominal exit site reduces peritoneal dialysis-related infections. Ther Apher Dial 2016;20:158–164.
Penner T, Crabtree JH. Peritoneal dialysis catheters with back exit sites. Perit Dial Int 2013;33:93–96.
Twardowski ZJ, Nichols WK, Nolph KD, Khanna R. Swan neck presternal («bath tub») catheter for peritoneal dialysis. Adv Perit Dial 1992;8:316–324.
Twardowski ZJ, Prowant BF, Nichols WK, Nolph KD, Khanna R. Six-year experience with swan neck presternal peritoneal dialysis catheter. Perit Dial Int 1998; 18:598–602.
Zimmerman DG. Presternal catheter design – an opportunity to capitalize on catheter immobilization. Adv Perit Dial 2010;26:91–95.
1. Выбор катетера
1.1. Выбранный катетер для перитонеального диализа должен иметь соответствующее положение дистального сегмента катетера и место его выхода с минимизацией риска инфекции, являться легковидимым и доступным пациенту, что в результате приводит к минимальной нагрузке на сегмент катетера в туннеле брюшной стенки.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Blake P. Drain pain, overfill, and how they are connected. Perit Dial Int 2014;34:342–344.
Crabtree JH, Burchette RJ, Siddiqi NA. Optimal peritoneal dialysis catheter type and exit-site location: an anthropometric analysis. ASAIO J 2005;51:743–747.
Crabtree JH, Burchette RJ. Prospective comparison of downward and lateral peritoneal dialysis catheter tunnel-tract and exit-site directions. Perit Dial Int 2006;26:677–683.
Crabtree JH. Selected best demonstrated practices in peritoneal dialysis access. Kidney Int 2006;70:S27–37.
Helfrich GB, Winchester JF. What is the best technique for implantation of a peritoneal dialysis catheter? Perit Dial Bull 1982;2:132–133.
Twardowski ZJ, Prowant BF, Nichols WK, Nolph KD, Khanna R. Six-year experience with swan neck presternal peritoneal dialysis catheter. Perit Dial Int 1998;18:598–602.
Twardowski ZJ, Tully RJ, Ersoy F, Dedhia NM. Computerized tomography with and without intraperitoneal contrast for determination of intraab-dominal fluid distribution and diagnosis of complications in peritoneal dialysis patients. ASAIO Transactions 1990;36:95–103.
Twardowski ZJ. Peritoneal catheter placement and management. In: Massry SG, Suki WN, eds. Therapy of Renal Disease and Related Disorders. Dordrecht: Kluwer Academic; 1997:953–979.
1.2. Рекомендуем информировать команду, осуществляющую формирование доступа для перитонеального диализа, о базовом перечне катетеров, что позволит выбрать наиболее подходящий тип катетера, исходя из конституционных особенностей и клинического состояния пациента.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
1.3. Рекомендуем команде, осуществляющей формирование доступа для перитонеального диализа, разработать протокол предоперационного картирования для выбора наиболее подходящего типа катетера из своего перечня.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Crabtree JH, Piraino B, Gellens M, Guest S, Firanek CA, Mancini A. Preoperative mapping to determine the most appropriate catheter type, insertion site, and exit-site location. In: Access Care and Complications Management Update, 2017. Care of the Adult Patient on Peritoneal Dialysis. Deerfield, IL: Baxter Healthcare Corporation; 2017:62–67.
Crabtree JH. Construction and use of stencils in planning for peritoneal dialysis catheter implantation. Perit Dial Int 2003; 23:395–402.
2. Процедура имплантации катетера для перитонеального диализа
2.1. Соблюдение ряда рекомендаций по подготовке пациентов к вмешательству и имплантации перитонеального катетера имеет большое значение для создания успешного долгосрочного доступа к перитонеальному диализу независимо от метода имплантации катетера.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Таблица 1 ПД
2.2. Выбор метода имплантации катетера для перитонеального диализа должен основываться на конституционных особенностях и клиническом состоянии пациента, ресурсах медицинской организации, знаниях и опыте оператора.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Таблица 2 ПД
2.3. При лапароскопической технике имплантации катетера для перитонеального диализа рекомендуем применение современных прогрессивных технологий, способных сводить к минимуму риск механических осложнений.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Attaluri V, Lebeis C, Brethauer S, Rosenblatt S. Advanced laparoscopic techniques significantly improve function of peritoneal dialysis catheters. J Am Coll Surg 2010; 211(6):699–704.
Bar-Zohar D, Sagie B, Lubezky N, Blum M, Klausner J, Abu-Abeid S. Laparoscopic implantation of the Tenckhoff catheter for the treatment of end-stage renal failure and congestive heart failure: experience with the pelvic fixation stitch. IMAJ 2006;8:174–178.
Bircan HY, Kulah E. Effects of a novel peritoneal dialysis: the open versus laparoscopic preperitoneal tunneling technique. Ther Apher Dial 2016;20:66–72.
Crabtree JH, Burchette RJ. Effective use of laparoscopy for long-term peritoneal dialysis access. Am J Surg 2009;198:135–141.
Crabtree JH, Fishman A. A laparoscopic method for optimal peritoneal dialysis access. Am Surg 2005;71(2):135–143.
Crabtree JH, Fishman A. Laparoscopic epiplopexy of the greater omentum and epiploic appendices in the salvaging of dysfunctional peritoneal dialysis catheters. Surg Laparosc Endosc 1996;6:176–180.
Goh YH. Omental folding: a novel laparoscopic technique for salvaging peritoneal dialysis catheters. Perit Dial Int 2008;28:626–631.
Gunes ME, Uzum G, Koc O, Duzkoylu Y, Kucukyilmaz M, Sari YS, et al. A modified method in laparoscopic peritoneal catheter implantation: the combination of preperitoneal tunneling and pelvic fixation. ISRN Surg 2013; 2013:248126.
Harissis HV, Katsios CS, Koliousi EL, Ikonomoub MG, Siamopoulos KC, Fatouros M, et al. A new simplified one-port laparoscopic technique of peritoneal dialysis catheter placement with intra-abdominal fixation. Am J Surg 2006;192:125–129.
Heithold DL, Duncan TD, White JG, Lucas GW. Laparoscopic placement of peritoneal dialysis catheters with medical umbilical fold tunnel formation. Surg Rounds 1997;20:310–314.
Jwo SC, Chen KS, Lee CC, Chen HY. Prospective randomized study for comparison of open surgery with laparoscopic-assisted placement of Tenckhoff peritoneal dialysis catheter – a single-center experience and literature review. J Surg Res 2010;159:489–496.
Klein Z, Magen E, Fishman A, Korzets Z. Laparoscopic salpingectomy: definitive treatment for peritoneal dialysis catheter obstruction caused by oviductal fimbriae. J Laparoendosc Adv Surg Tech A 2003;13:65–68.
Krezalek MA, Bonamici N, Lapin B, Carbray J, Velasco J, Denham W, et al. Laparoscopic peritoneal dialysis catheter insertion using rectus sheath tunnel and selective omentopexy significantly reduces catheter dysfunction and increases peritoneal dialysis longevity. Surgery 2016; 160(4):924–935.
Lu CT, Watson DI, Elias TJ, Faull RJ, Clarkson AR, Bannister KM. Laparoscopic placement of peritoneal dialysis catheters: 7 years experience. ANZ J Surg 2003;73:109–111.
Mo M, Ju Y, Zhang W, Pan J, Zheng Q, Chen J, et al. Peritoneal dialysis catheter emplacement by advanced laparoscopy: 8-year experience from a medical center in China. Sci Rep 2017;27(1):9097.
Ogunc G. Minilaparoscopic extraperitoneal tunneling with omentopexy: a new technique for CAPD catheter placement. Perit Dial Int 2005; 25(6):551–555.
Santarelli S, Zeiler M, Marinelli R, Monteburini T, Federico A, Ceraudo E. Videolaparoscopy as rescue therapy and placement of peritoneal dialysis catheters: a thirty-two case single-centre experience. Nephrol Dial Transplant 2006;21:1348–1354.
Wright MJ, Bel’eed K, Johnson BF, Eadington DW, Sellars L, Farr MJ. Randomized prospective comparison of laparoscopic and open peritoneal dialysis catheter insertion. Perit Dial 1999;19:372–375.
2.4. Предполагаем использовать визуализацию (УЗИ и/или флюороскопию) для улучшения результатов и минимизации осложнений при чрескожном введении катетеров для перитонеального диализа с помощью иглы и проводника.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Abdel-Aal AK, Dybbro P, Hathaway P, Guest S, Neuwirth M, Krishnamurthy V. Best practices consensus protocol for peritoneal dialysis catheter place¬ment by interventional radiologists. Perit Dial Int 2014;34:481–493.
Shanmugalingam R, Makris A, Hassan HC, Li Y, DeGuzman I, Nandakoban H, et al. The utility of sonographic assessment in selecting patients for percutaneous insertion of peritoneal dialysis catheter. Perit Dial Int 2017; 37:434–442.
3. Периоперативные манипуляции с катетером для перитонеального диализа
3.1. Предлагаем проводить пробное промывание катетера для перитонеального диализа достаточным объемом раствора до окончательной установки на место, чтобы наглядно убедиться в беспрепятственном притоке и оттоке.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Cho Y, Boudville N, Palmer SC, Chow JSF, Hawley CM, Jose MD, et al. Prac¬tice of peritoneal dialysis catheter flushing in Australia and New Zealand: multi-center cross-sectional survey. Perit Dial Int 2018;38:98–103.
Wallace EL, Fissell RB, Golper TA, Blake PG, Lewin AM, Oliver MJ, et al. Catheter insertion and perioperative practices within the ISPD North American research consortium. Perit Dial Int 2016;36:382–386.
3.2. Предлагаем варьировать промывку катетера для перитонеального диализа после операции в зависимости от индивидуального состояния пациента. Временные рамки и частота промывок зависят от наличия или отсутствия крови в пробах жидкости после промывания во время установки катетера или наличия персистирующего геморрагического экссудата в жидкости после промывания в послеоперационном периоде.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Crabtree JH, Burchette RJ. Peritoneal dialysis access and start practices that affect dialysate leak and technique failure: acts of commission and omission. Perit Dial Int 2017;37:358–361.
Gadallah MF, Torres–Rivera C, Ramdeen G, Myrick S, Habashi S, Andrews G. Relationship between intraperitoneal bleeding, adhesions, and peritoneal dialysis catheter failure: a method of prevention. Adv Perit Dial 2001;17:127–129.
Ranganathan D, John GT, Yeoh E, Williams N, O’Loughlin B, Han T, et al. A randomized controlled trial to determine the appropriate time to initiate peritoneal dialysis after insertion of catheter (timely PD study). Perit Dial Int 2017;37:420–428. 130.
3.3. Во время процедуры имплантации катетера для перитонеального диализа предлагаем присоединить рекомендуемый в конкретном центре адаптер катетера и удлинитель.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
3.4. Предлагаем использовать неокклюзионную марлевую хирургическую повязку по размеру, достаточному для иммобилизации катетера для перитонеального диализа, дренирования, предотвращения травм и загрязнения места выхода катетера.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Kopriva-Altfahrt G, Konig P,MundleM, Prischl F, Roob JM,WiesholzerM, et al. Exit-site care in Austrian peritoneal dialysis centers – a nationwide survey. Perit Dial Int 2009;29:330–339.
Li PK, Szeto CC, Piraino B, de Arteaga J, Fan S, Figueiredo AE, et al. ISPD peritonitis recommendations: 2016 update on prevention and treatment. Perit Dial Int 2016; 36:481–508.
Prowant BF, Warady BA, Nolph KD. Peritoneal dialysis catheter exit-site care: results of an international study. Perit Dial Int 1993;13:149–154.
Szeto CC, Li PK, Johnson DW, Bernardini J, Dong J, Figueiredo AE, et al. ISPD catheter-related infection recommendations: 2017 UPDATE. Perit Dial Int 2017;37:141–154.
3.5. Предлагаем по возможности рекомендовать послеоперационные перевязки выполнять только опытными медсестрами, работающими с пациентами, получающими медицинскую помощь методами перитонеального диализа.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
4. Начало лечения методом перитонеального диализа
4.1. Рекомендуем время от имплантации катетера для перитонеального диализа до начала запланированного лечения ограничить по крайней мере двумя неделями.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Li PK, Szeto CC, Piraino B, de Arteaga J, Fan S, Figueiredo AE, et al. ISPD peritonitis recommendations: 2016 UPDATE on prevention and treatment. Perit Dial Int 2016;36:481–508.
Povlsen JV, Ivarsen P. How to start the late-referred ESRD patient urgently on chronic APD. Nephrol Dial Transplant 2006; 26(Suppl 2):S56–59.
Ranganathan D, John GT, Yeoh E, Williams N, O’Loughlin B, Han T, et al. A randomized controlled trial to determine the appropriate time to initiate peritoneal dialysis after insertion of catheter (timely PD study). Perit Dial Int 2017;37:420–428.
Szeto CC, Li PK, Johnson DW, Bernardini J, Dong J, Figueiredo AE, et al. ISPD catheter-related infection recommendations: 2017 UPDATE. Perit Dial Int 2017;37:141–154.
4.2. Рекомендуем модифицировать время начала лечения менее чем через две недели после имплантации катетера, если необходимо экстренное или неотложное оказание медицинской помощи методами перитонеального диализа с использованием обменов с небольшими объемами в положении лежа на спине.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Dejardin A, Robert A, Coffin E. Intraperitoneal pressure in PD patients: relationship to intraperitoneal volume, body size and PD-related complications. Nephrol Dial Transplant 2007;5:1437–1444.
Pai MF, Yang JY, Chen HY, Hsu SP, Chiu YL, Wu HY, et al. Comparing long-term outcomes between early and delayed initiation of peritoneal dialysis following catheter implantation. Renal Failure 2016;38:875–81.
Povlsen JV, Sorensen AB, Ivarsen P. Unplanned start on peritoneal dialysis right after PD catheter implantation for older people with end-stage renal disease. Perit Dial Int 2015;35:622–624.
See EJ, Cho Y, Hawley C, Jaffrey LR, Johnson DW. Early and late patient outcomes in urgent-start peritoneal dialysis. Perit Dial Int 2016;37:414–419.
5. Инфекционные осложнения доступа для перитонеального диализа и лечения
5.1. Предлагаем сбривать поверхностную манжету катетера для перитонеального диализа при ее экструзии.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Debowski JA, Wærp C, Kjellevold SA, Abedini S. Cuff extrusion in peritoneal dialysis: single-centre experience with cuff-shaving procedure in five patients over a 4-year period. Clin Kidney J 2017;10:131–134.
5.2. Рекомендуем проводить ультразвуковое исследование трансмурального сегмента катетера для перитонеального диализа при хронической инфекции места выхода катетера, при инфекции в месте выхода катетера, медленно реагирующей на лечение, особенно в случаях, связанных со Staphylococcus aureus и Pseudomonas aeruginosa, и использовать эти данные для коррекции лечения.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Debowski JA, Wærp C, Kjellevold SA, Abedini S. Cuff extrusion in peritoneal dialysis: single-centre experience with cuff-shaving procedure in five patients over a 4-year period. Clin Kidney J 2017;10:131–134.
Plum J, Sudkamp S, Grabensee B. Results of ultrasound-assisted diagnosis of tunnel infections in continuous ambulatory peritoneal dialysis. Am J Kidney Dis 1994;23:99–104.
Szeto CC, Li PK, Johnson DW, Bernardini J, Dong J, Figueiredo AE, et al. ISPD catheter-related infection recommendations: 2017 UPDATE. Perit Dial Int 2017;37:141–154.
Twardowski ZJ, Prowant BF. Classification of normal and diseased exit sites. Perit Dial Int 1996;16(Suppl 3):S32–50.
5.3. Предлагаем при хронической инфекции места выхода катетера для перитонеального диализа выделить межманжеточный сегмент катетера и создать для него новый туннель до другого удовлетворяющего требованиям места выхода катетера, при этом при ультразвуковом исследовании не должна визуализироваться жидкость вокруг поверхностной манжеты катетера.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Crabtree JH. Peritoneal dialysis catheter splicing for distant relocation of poorly selected exit sites. Perit Dial Int 2005;25:192–195.
Fukazawa M, Matsushita K, Tanabe N, Mochizuki T, Hara T, Takeda M. A novel salvage technique that does not require catheter removal for exit-site infection. Perit Dial Int 2002;22:618–621.
Wu YM, Tsai MK, Chao SH, Tsai TJ, Chang KJ, Lee PH. Surgical management of refractory exit-site/tunnel infection of Tenckhoff catheter: technical innovations of partial replantation. Perit Dial Int 1999;19:451–454.
5.4. Рекомендуем удаление/сбривание манжеты или одновременную замену катетера для перитонеального диализа при клинических или ультразвуковых данных туннельной инфекции с визуализацией жидкости вокруг поверхностной манжеты и /или сегмента катетера между манжетами.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Crabtree JH, Burchette RJ. Surgical salvage of peritoneal dialysis catheters from chronic exit-site and tunnel infections. Am J Surg 2005;190:4–8. 149. Terawaki H, Nakano H, Ogura M, Kadomura M, Hosoya T, Nakayama M. Unroofing surgery with en bloc resection of the skin and tissues around the peripheral cuff. Perit Dial Int 2013;33:573–576.
5.5. Рекомендуем удаление катетера, перевод пациента на лечение методом гемодиализа и поэтапное повторное введение катетера для перитонеального диализа при клинических или ультразвуковых доказательствах туннельной инфекции с визуализацией жидкости вокруг глубокой манжеты или наличия сопутствующего перитонита.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Li PK, Szeto CC, Piraino B, de Arteaga J, Fan S, Figueiredo AE, et al. ISPD peritonitis recommendations: 2016 UPDATE on prevention and treatment. Perit Dial Int 2016;36:481–508.
Matuszkiewicz-Rowinska J. UPDATE on fungal peritonitis and its treatment. Perit Dial Int 2009; 29(Suppl 2):S161–165.
Miles R, Hawley CM, McDonald SP, Brown FG, Rosman JB, Wiggins KJ, et al. Predictors and outcomes of fungal peritonitis in peritoneal dialysis patients. Kidney Int 2009;76:622–628.
Ram R, Swarnalatha G, Dakshinamurty KV. Reinitiation of peritoneal dialysis after catheter removal for refractory peritonitis. J Nephrol 2014;27:445–449.
Szeto CC, Chow KM, Wong TY, Leung CB, Wang AY, Lui SF, et al. Feasibility of resuming peritoneal dialysis after severe peritonitis and Tenckhoff catheter removal. J Am Soc Nephrol 2002;13:1040–1045.
Troidle L, Gorban-Brennan N, Finkelstein FO. Outcome of patients on chronic peritoneal dialysis undergoing peritoneal catheter removal because of peritonitis. Adv Perit Dial 2005;21:98–101.
5.6. Рекомендуем одновременную замену катетера перитонеального диализа при рецидивирующем перитоните, вызванном стафилококками, если антибиотикотерапия устраняет абдоминальные симптомы и количество клеток в перитонеальной жидкости <100/мкл.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Crabtree JH, Siddiqi, RA. Simultaneous catheter replacement for infectious and mechanical complications without interruption of peritoneal dialysis. Perit Dial Int 2016;36:182–187.
Li PK, Szeto CC, Piraino B, de Arteaga J, Fan S, Figueiredo AE, et al. ISPD peritonitis recommendations: 2016 UPDATE on prevention and treatment. Perit Dial Int 2016;36:481–508.
Mitra A, Teitelbaum I. Is it safe to simultaneously remove and replace infected peritoneal dialysis catheters? Review of the literature and suggested guidelines. Adv Perit Dial 2003;19:255–259.
6. Перикатетерное протекание и лечение
6.1.Рекомендуем отложить начало лечения методами перитонеального диализа после установки катетера для перитонеального диализа, если это возможно, на 2 недели, чтобы минимизировать риск перикатетерного протекания.
Уровень достоверности доказательств III, уровень убедительности рекомендаций B
Diaz-Buxo JA, GewissingerWT. Single-cuff versus double-cuff Tenckhoff catheter. Perit Dial Bull 1984; 4(Suppl):S100–102.
Helfrich GB, Pechan BW, Alifani MR. Reduction in catheter complications with lateral placement. Perit Dial Bull 1983;3(Suppl):S2–4.
Holley JL, Bernardini J, Piraino B: Characteristics and outcome of peritoneal dialysate leaks and associated infections. Adv Perit Dial 1993;9:240–243.
Leblanc M, Ouimet D, Pichette V. Dialysate leaks in peritoneal dialysis. Semin Dial 2001;14:50–54.
Spence PA, Mathews RE, Khanna R, Oreopoulos DG. Improved results with a paramedian technique for the insertion of peritoneal dialysis catheters. Surg Gynecol Obstet 1985;161:585–587.
Twardowski ZJ, Khanna R, Nolph KD, Scalamogna A, Metzler MH, Schneider TW, et al. Intraabdominal pressures during natural activities in patients treated with continuous ambulatory peritoneal dialysis. Nephron 1986;44:129–135.
Tzamaloukas AH, Gibel LJ, Eisenberg B, Goldman RS, Kanig SP, Zager PG, et al. Early and late peritoneal dialysis leaks in patients on CAPD. Adv Perit Dial 1990;6:64–70.
Winchester JF, Kriger FL. Fluid leaks: prevention and treatment. Perit Dial Int 1994;14(Suppl 3):S43–48.
6.2. Рекомендуем при экстренном и неотложном начале лечения методами перитонеального диализа менее чем через 2 недели после установки катетера схема лечения включать интермиттирующие обмены небольшими объемами в положении лежа на спине, при этом минимизировать риск перикатетерного протекания; брюшная полость остается «сухой» во время периодов между заливками.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
Tzamaloukas AH, Gibel LJ, Eisenberg B, Goldman RS, Kanig SP, Zager PG, et al. Early and late peritoneal dialysis leaks in patients on CAPD. Adv Perit Dial 1990; 6:64–70.
6.3. Рекомендуем использовать КТ-перитонеографию или перитонеальную сцинтиграфию для определения места и границ при подозрении на перикатетерное протекание.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Bargman JM. Complications of peritoneal dialysis related to increase intraabdominal pressure. Kidney Int 1993;43:S75–80.
Crabtree JH. Rescue and salvage procedures for mechanical and infectious complications of peritoneal dialysis. Int J Artif Organs 2006;29:67–84.
Holley JL, Bernardini J, Piraino B: Characteristics and outcome of peritoneal dialysate leaks and associated infections. Adv Perit Dial 1993;9:240–243.
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
Juergensen PH, Rizvi H, Caride VJ, Kliger AS, Finkelstein FO. Value of scintigraphy in chronic peritoneal dialysis patients. Kidney Int 1999;55:1111–1119.
Leblanc M, Ouimet D, Pichette V. Dialysate leaks in peritoneal dialysis. Semin Dial 2001;14:50–54.
Mak SK, Nyunt K, Wong PN, Lo KY, Tong GM, Tai YP, et al. Long-term followup ofthoracoscopic pleurodesisfor hydrothorax complicating peritoneal dialysis. Ann Thorac Surg 2002;74:218–221.
Nomoto Y, Suga T, Nakajima K, Sakai H, Osawa G, Ota K, et al. Acute hydrothorax in continuous ambulatory peritoneal dialysis – a collaborative study of 161 centers. Am J Nephrol 1989;9:363–367.
Tang S, Chui WH, Tang AW, Li FK, Chau WS, Ho YW, et al. Video-assisted thoracoscopic talc pleurodesis is effective for maintenance of peritoneal dialysis in acute hydrothorax complicating peritoneal dialysis. Nephrol Dial Transplant 2003;18:804–808.
7. Дисфункция потока через катетер для перитонеального диализа и лечения
7.1. Диагностические исследования и лечение дисфункции потока через катетер для перитонеального диализа должны проходить в логическом порядке – от консервативных или неинвазивных подходов к более агрессивным вмешательствам.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Hutchinson PJ, Chand DH. Use of tissue plasminogen activator in obstructed peritoneal dialysis catheters. Dial Transplant 2001;30:104–108.
Kaplan SA, Wein AJ, Staskin DR, Roehrborn CG, Steers WD. Urinary retention and post-void residual urine in men: separating truth from tradition. J Urol 2008;180:47–54.
Kelly CE. Evaluation of voiding dysfunction and measurement of bladder volume. Rev Urol 2004;6(Suppl 1):S32–37.
Sahani MM, Mukhtar KN, Boorgu R, Leehey DJ, Popli S, Ing TS. Tissue plasminogen activator can effectively declot peritoneal dialysis catheters. [Letter] Am J Kidney Dis 2000;36:675.
Singharetnam W, Holley JL. Acute treatment of constipation may lead to transmural migration of bacteria resulting in gram-negative, polymicrobial, or fungal peritonitis. Perit Dial Int 1996;16:423–425.
Uchiyama K, Kamijo Y, Yoshida R, Nakatsuka M, Ishibashi Y. Importance of neurogenic bladder as cause of drainage failure. Perit Dial Int 2016;36:232–233.
Vijt D, Castro MJ, Endall G, Lindley E, Elseviers M. Post insertion catheter care in peritoneal dialysis (PD) centres across Europe – Part 2: complication rates and individual patient outcomes. EDTNA ERCA J 2004;30:91–96.
Zorzanello MM, Fleming WJ, Prowant BE. Use of tissue plasminogen activator in peritoneal dialysis catheters: a literature review and one center’s experience. Nephrol Nurs J 2004;31:534–7.
7.2. Выбор вмешательства при дисфункции потока через катетер для перитонеального диализа (радиологические манипуляции, лапароскопическое лечение или одновременная замена катетера) должен основываться на факторах, связанных с пациентом, ресурсах учреждения и на опыте оператора.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Alabi A, Dholakia S, Ablorsu E. The role of laparoscopic surgery in the management of a malfunctioning catheter. Ann R Coll Surg Eng.l 2014;96:593–596.
Crabtree JH, Burchette RJ. Effective use of laparoscopy for long-term peritoneal dialysis access. Am J Surg. 2009;198:135–141.
Crabtree JH, Burchette RJ. Peritoneal dialysis catheter embedment: surgical considerations, expectations, and complications. Am J Surg. 2013;206:464–471.
Crabtree JH, Siddiqi, RA. Simultaneous catheter replacement for infectious and mechanical complications without interruption of peritoneal dialysis. Perit Dial Int 2016;36:182–187.
Crabtree JH. Rescue and salvage procedures for mechanical and infectious complications of peritoneal dialysis. Int J Artif Organs. 2006;29:67–84.
Harissis HV, Katsios CS, Koliousi EL, Ikonomoub MG, Siamopoulos KC, Fatouros M, et al. A new simplified one-port laparoscopic technique of peritoneal dialysis catheter placementwith intra-abdominal fixation. Am J Surg. 2006;192:125–129.
Kim HJ, Lee TW, Ihm CG, Kim MJ. Use of fluoroscopy-guided wire manipulation and/or laparoscopic surgery in the repair of malfunctioning peritoneal dialysis catheters. Am J Nephrol. 2002;22:532–538.
Klein Z, Magen E, Fishman A, Korzets Z. Laparoscopic salpingectomy: definitive treatment for peritoneal dialysis catheter obstruction caused by oviductal fimbriae. J Laparoendosc Adv Surg Tech A. 2003;13:65–68.
Krezalek MA, Bonamici N, Lapin B, Carbray J, Velasco J, Denham W, et al. Laparoscopic peritoneal dialysis catheter insertion using rectus sheath tunnel and selective omentopexy significantly reduces catheter dysfunction and increases peritoneal dialysis longevity. Surgery. 2016;160(4):924–935.
Kwon YH, Kwon SH, Oh JH, Jeong KH, Lee TW. Fluoroscopic guide wire manipulation of malfunctioning peritoneal dialysis catheters initially placed by interventional radiologists. J Vasc Interv Radiol. 2014;25:904–910.
Miller M, McCormick B, Lavoie S, Biyani M, Zimmerman D. Fluoroscopic manipulation of peritoneal dialysis catheters: outcomes and factors associated with successful manipulation. Clin J Am Soc Nephrol. 2012;7:795–800.
Ogunc G. Malfunctioning peritoneal dialysis catheter and accompanying surgical pathology repaired by laparoscopic surgery. Peri Dial Int. 2002;22:454–462.
Ovnat A, Dukhno O, Pinsk I, Peiser J, Levy I. The laparoscopic option in the management of peritoneal dialysis catheter revision. Surg Endosc. 2002;16:698–699.
OzyerU,HarmanA,Aytekin C,Boyvat F,Ozdemir N. Correction of displaced peritoneal dialysis catheters with an angular stiff rod. Acta Radiol. 2009;50:139–143.
Savader SJ, Lund G, Scheel PJ, Prescott C, Feeley N, Singh H, et al. Guide wire directed manipulation of malfunctioning peritoneal dialysis catheters: a critical analysis. J Vasc Interv Radiol. 1997;8:957–963.
Simons ME, Pron G, Voros M, VanderburghLC, Rao PS, Oreopoulos DG. Fluoroscopically guided manipulation of malfunctioning peritoneal dialysis catheters. Perit Dial Int. 1999;19:544–549.
Usha K, Ponferrada L, Prowant BF, Twardowski, ZJ. Repair of chronic peritoneal dialysis catheter. Perit Dial Int. 1998; 18:419–423.
Zoland MP, Loubeau JM, Krapf R, Zabetakis PM. A simplified laparoscopic salvage technique for malfunctioning chronic peritoneal dialysis catheters. Perit Dial Int. 1997;17:610–612.
8. Удаление катетера для перитонеального диализа
8.1. Катетеры могут быть удалены с помощью открытой хирургической диссекции или «техники вытягивания».
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Kahveci A, Ari E, Asicioglu E, Arikan H, Tuglular S, Ozener C. Peritoneal dialysis catheter removal by nephrologists: technical aspect from a single center. Perit Dial Int 2010;30:570–572.
8.2. Предлагаем выполнять открытое хирургическое вмешательство для удаления неповрежденных дакроновых манжет катетера, удлинителя катетера с титановым коннектором при туннельной инфекции или перитоните, связанных с инфекцией катетера для перитонеального диализа.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Elkabir JJ, Riaz AA, Agarwal SK, Williams G. Delayed complications following Tenckhoff catheter removal. Nephrol Dial Transplant. 1999;14:1550–1552.
Korzets Z, Hasdan G, Bulkan G, Klein E, Bernheim J, Shpitz B. Early postoperative complications of removal of Tenckhoff peritoneal dialysis catheter. Perit Dial Int. 2000;20(6):789–791.
8.3. Полагаем, что «техника вытягивания» лучше всего подходит в случае, если удаление катетера для перитонеального диализа проводится по неинфекционным показаниям, при этом отмечается минимальный риск инфицирования, если дакроновые манжеты остаются в тканях по тем или иным причинам.
Уровень достоверности доказательств III, уровень убедительности рекомендаций C
Quiroga IM, Baboo R, Lord RH, Darby CR. Tenckhoff catheters post-renal transplantation: the ‘pull’ technique? Nephrol Dial Transplant. 2001;16:2079–2081.
Grieff M,Mamo E, Scroggins G, Kurchin A. The ‘pull’ technique for removal of peritoneal dialysis catheters: a call for re-evaluation of practice standards. Perit Dial Int. 2017;37:225–229.
9. Вторичное введение катетера для перитонеального диализа
9.1. Предлагаем вторичное введение катетера для перитонеального диализа, когда функция почек достаточно улучшилась для того, чтобы остановить диализ, но не ожидается долгосрочного ее восстановления при ранее нормальной функции потока катетера для перитонеального диализа.
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Crabtree JH. Secondary embedding of peritoneal dialysis catheters. Perit Dial Int. 2008;28:203–206.
Sakurada T, Kaneshiro N, Taki Y, Kojima S, Koitabashi K, Sueki S, et al. Long-term prognosis of peritoneal dialysis patients with a re-embedded catheter. Adv Perit Dial. 2017;33:31–34.
10. Оценка доступа для перитонеального диализа
10.1. Рекомендуем проводить оценку результатов имплантации катетера для перитонеального диализа не реже 1 раза в год в рамках междисциплинарного совещания персонала, оказывающего медицинскую помощь методами перитонеального диализа, включая присутствие хирургов.
Уровень достоверности доказательств I, уровень убедительности рекомендаций B
Crabtree JH, Burchette RJ. Effective use of laparoscopy for long-term peritoneal dialysis access. Am J Surg. 2009;198:135–141.
Crabtree JH, Fishman A. A laparoscopic method for optimal peritoneal dialysis access. Am Surg. 2005;71(2):135–143.
Ivers NM, Grimshaw JM, Jamtvedt G, Flottorp S, O’Brien MA, French SD, et al. Growing literature, stagnant science? Systematic review, metaregression and cumulative analysis of audit and feedback interventions in health care. J Gen Intern Med. 2014;29:1534–1541.
Jwo SC, Chen KS, Lee CC, Chen HY. Prospective randomized study for comparison of open surgery with laparoscopic-assisted placement of Tenckhoff peritoneal dialysis catheter – a single-center experience and literature review. J Surg Res. 2010;4159:489–496.
Krezalek MA, Bonamici N, Lapin B, Carbray J, Velasco J, Denham W, et al. Laparoscopic peritoneal dialysis catheter insertion using rectus sheath tunnel and selective omentopexy significantly reduces catheter dysfunction and increases peritoneal dialysis longevity. Surgery. 2016;160(4):924–935.
Maher E, Wolley MJ, Abbas SA, Hawkins SP, Marshall MR. Fluoroscopic versus laparoscopic implantation of peritoneal dialysis catheters: a retrospective cohort study. J Vasc Interv Radiol. 2014;25:895–903.
Mo M, Ju Y, Zhang W, Pan J, Zheng Q, Chen J, et al. Peritoneal dialysis catheter emplacement by advanced laparoscopy: 8-year experience from a medical center in China. Sci Rep. 2017;27(1):9097.
Moon JY, Song S, Jung KH, Park M, Lee SH, Ihm CG, et al. Fluoroscopically guided peritoneal dialysis catheter placement: long-term results from a single center. Perit Dial Int. 2008;28:163–169.
Sethna CB, Bryant K, Munshi R, Warady BA, Richardson T, Lawlor J, et al. Risk factors for and outcomes of catheter-associated peritonitis in children: the SCOPE collaborative. Clin J Am Soc Nephrol. 2016;11:1590–1596.
Soontrapornchai P, Simapatanapong T. Comparison of open and laparoscopic secure placement of peritoneal dialysis catheters. Surg Endosc. 2005;19:137–139.
Tullavardhana T, Akranurakkul P, Ungkitphaiboon W, Songfish D. Surgical versus percutaneous techniques for peritoneal dialysis catheter placement: a meta-analysis of the outcomes. Ann Med Surg (Lond). 2016;10:11–18.
Voss D, Hawkins S, Poole G, Marshall M. Radiological versus surgical implantation of first catheter for peritoneal dialysis: a randomized noninferiority trial. Nephrol Dial Transplant. 2012;27:4196–204
Wright MJ, Bel’eed K, Johnson BF, Eadington DW, Sellars L, Farr MJ. Randomized prospective comparison oflaparoscopic and open peritoneal dialysis catheter insertion. Perit Dial. 1999;19:372–375.
10.2. Предлагаем целевые показатели, специфичные для оценки доступа для перитонеального диализа
Уровень достоверности доказательств II, уровень убедительности рекомендаций C
10.2.1. Проходимость катетера через 12 месяцев >95% при расширенном лапароскопическом методе введения катетера и 80% для всех других методов введения катетера.
10.2.2. Инфекция в месте выхода катетера/туннельная инфекция в течение 30 дней после введения катетера <5%.
10.2.3. Перитонит в течение 30 дней после введения катетера <5%.
10.2.4. Повреждение внутренних органов (кишечник, мочевой пузырь, паренхиматозные органы) <1%.
10.2.5. Значимое кровотечение, требующее переливания компонентов крови или хирургического вмешательства <1%.
Crabtree JH, Fishman A. A laparoscopic method for optimal peritoneal dialysis access. Am Surg. 2005;71(2):135–143.
Dunne N, Booth MI, Dehn TC. Establishing pneumoperitoneum: Verres or Hasson? The debate continues. Ann R Coll Surg Engl. 2011;93:22–24.
Gadallah MF, Pervez A, el-Shahawy MA, Sorrells D, Zibari G, McDonald J. Peritoneoscopic versus surgical placement of peritoneal dialysis catheters: a prospective randomized study on outcome. Am J Kidney Dis. 1999;33:118–122.
Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections, 1992; a modification of CDC definitions of surgical wound infections. Infection Control Hosp Epidemiol. 1992;13:606–608.
Krezalek MA, Bonamici N, Lapin B, Carbray J, Velasco J, Denham W, et al. Laparoscopic peritoneal dialysis catheter insertion using rectus sheath tunnel and selective omentopexy significantly reduces catheter dysfunction and increases peritoneal dialysis longevity. Surgery. 2016;160(4):924–935.
Medani S, Hussein W, Shantier M, Flynn R, Wall C, Mellotte G. Comparison of percutaneous and open surgical techniques for first-time peritoneal dialysis catheter placement in the unbreached peritoneum. Perit Dial Int. 2015;35:576–585.
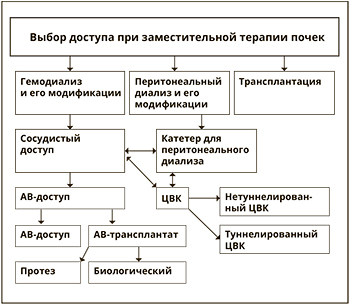
Mohamed A, Bennett M, Gomez L, Massingill E, Le L, Peden E, et al. Laparoscopic peritoneal dialysis surgery is safe and effective in patients with prior abdominal surgery. Ann Vasc Surg. 2018;53:133–138.
Moon JY, Song S, Jung KH, Park M, Lee SH, Ihm CG, et al. Fluoroscopically guided peritoneal dialysis catheter placement: long-term results from a single center. Perit Dial Int. 2008;28:163–169.
Riara S, Abdulhadi M, Day C, Prasad B. Accidental insertion of a peritoneal dialysis catheter in the urinary bladder. Case Rep Nephrol Dial. 2018;8:76–81.
10.3. Предлагаем случаи перикатетерного протекания в течение 30 дней после введения катетера регистрировать отдельно при раннем начале ПД (<14 дней) и позднем начале (≥ 14 дней).
Уровень достоверности доказательств V, уровень убедительности рекомендаций C
Gadallah MF, Pervez A, el-Shahawy MA, Sorrells D, Zibari G, McDonald J. Peritoneoscopic versus surgical placement of peritoneal dialysis catheters: a prospective randomized study on outcome. Am J Kidney Dis. 1999;33:118–122.
Jwo SC, Chen KS, Lee CC, Chen HY. Prospective randomized study for comparison of open surgery with laparoscopic-assisted placement of Tenckhoff peritoneal dialysis catheter – a single-center experience and literature review. J Surg Res. 2010;159:489–496.
Leblanc M, Ouimet D, Pichette V. Dialysate leaks in peritoneal dialysis. Semin Dial 2001;14:50–54.
Povlsen JV, Ivarsen P. How to start the late-referred ESRD patient urgently on chronic APD. Nephrol Dial Transplant. 2006;26(Suppl 2):S56–59.
Ranganathan D, John GT, Yeoh E, Williams N, O’Loughlin B, Han T, et al. A randomized controlled trial to determine the appropriate time to initiate peritoneal dialysis after insertion of catheter (timely PD study). Perit Dial Int. 2017;37:420–428.
See EJ, Cho Y, Hawley C, Jaffrey LR, Johnson DW. Early and late patient outcomes in urgent-start peritoneal dialysis. Perit Dial Int. 2016;37:414–419.
Таблица 1 ПД
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
Подготовка пациентов к вмешательству и имплантации перитонеального катетера
• Предоперационная оценка пациента, проводимая междисциплинарной командой специалистов по формированию доступа для перитонеального диализа; выбор наиболее подходящего типа катетера, техники имплантации, места введения и места выхода катетера для ПД.
Crabtree JH, Burchette RJ, Siddiqi NA. Optimal peritoneal dialysis catheter type and exit-site location: an anthropometric analysis. ASAIO J. 2005;51:743–747.
• Подготовка кишечника для предотвращения периоперационной констипации.
Vijt D, Castro MJ, Endall G, Lindley E, Elseviers M. Post insertion cath¬eter care in peritoneal dialysis (PD) centres across Europe – Part 2: complication rates and individual patient outcomes. EDTNA ERCA J. 2004;30:91–96.
Singharetnam W, Holley JL. Acute treatment of constipation may lead to transmural migration of bacteria resulting in gram-negative, polymicro¬bial, or fungal peritonitis. Perit Dial Int. 1996;16:423–425.
• В день процедуры принять душ с обработкой мылом, содержащим хлоргексидин, участка тела, где планируется хирургическое вмешательство.
• При необходимости удаления волос использовать электрические машинки для стрижки.
Leaper D, Burman-Roy S, Palanca A, Cullen K, Worster D, Gautam-Aitken E, et al. Prevention and treatment of surgical site infection: summary of NICE guidance. BMJ. 2008;337:a1924.
• Опорожнить мочевой пузырь перед вмешательством, в противном случае следует установить катетер Фолея.
Rouse J, Walker R, Packer S. Inadvertent intravesical insertion of a Tenckhoff catheter. Perit Dial Int. 1996;16:186–187.
• Профилактическая предоперационная разовая доза антибиотика с антистафилококковой активностью.
• Gadallah MF, Ramdeen G, Mignone J, Patel D, Mitchell L, Tatro S. Role of preoperative antibiotic prophylaxis in preventing postoperative perito¬nitis in newly placed peritoneal dialysis catheters. Am J Kidney Dis. 2000;36:1014–1019.
• При хирургическом вмешательстве персонал операционной должен использовать медицинские шапочки, маски, стерильные костюмы и перчатки.
Leaper D, Burman-Roy S, Palanca A, Cullen K, Worster D, Gautam-Aitken E, et al. Prevention and treatment of surgical site infection: summary of NICE guidance. BMJ. 2008;337:a1924.
• Локальное место для вмешательства предварительно обрабатывается антисептическими средствами, операционное поле обкладывается стерильными простынями с прорезью или пеленками.
Leaper D, Burman-Roy S, Palanca A, Cullen K, Worster D, Gautam-Aitken E, et al. Prevention and treatment of surgical site infection: summary of NICE guidance. BMJ. 2008;337:a1924.
• Катетер для перитонеального диализа ополаскивают и промывают физиологическим раствором под давлением, и воздух выдавливают из дакроновых манжет путем скручивания манжет между пальцами.
Abdel-Aal AK, Dybbro P, Hathaway P, Guest S, Neuwirth M, Krishnamurthy V. Best practices consensus protocol for peritoneal dialysis catheter place¬ment by interventional radiologists. Perit Dial Int. 2014;34:481–493.
• Рекомендовано парамедиальное введение катетера для перитонеального диализа через прямую мышцу с расположением глубокой манжетой катетера внутри или под прямой мышцей.
Helfrich GB, Pechan BW, Alifani MR. Reduction in catheter complications with lateral placement. Perit Dial Bull. 1983;3(Suppl):S2–4.
Lovinggood JP. Peritoneal catheter implantation for CAPD. Perit Dial Bull 1984; 4:106–109.
Spence PA, Mathews RE, Khanna R, Oreopoulos DG. Improved results with a paramedian technique for the insertion of peritoneal dialysis catheters. Surg Gynecol Obstet. 1985;161:585–587.
• Расположение дистального сегмента катетера для перитонеального диализа должно быть в тазу.
Twardowski ZJ. Peritoneal catheter placement and management. In: Massry SG, Suki WN, eds. Therapy of Renal Disease and Related Disorders. Dordrecht: Kluwer Academic. 1997:953–979.
• Рекомендуется наложение швов вокруг катетера для перитонеального диализа на уровне брюшины и заднего и/или переднего влагалища прямой мышцы живота.
Chow KM, Szeto CC, Leung CB, Kwan BC, Pang WF, Li PK. Tenckhoff catheter insertion by nephrologists: open dissection technique. Perit Dial Int. 2010; 30:524–527.
Crabtree JH, Burchette RJ. Effective use of laparoscopy for long-term peritoneal dialysis access. Am J Surg. 2009;198:135–141.
Jo YI, Shin SK, Lee JH, Song JO, Park JH. Immediate initiation of CAPD following percutaneous catheter placement without break-in procedure. Perit Dial Int. 2007;27:179–183.
Kang SH, Do JY, Cho KH, Park JW, Yoon KW. Blind peritoneal catheter placement with a Tenckhoff trocar by nephrologists: a single-center experience. Nephrology. 2012;17:141–147.
Sharma AP, Mandhani A, Daniel SP, Filler G. Shorter break-in period is a viable option with tighter PD catheter securing during insertion. Nephrology. 2008;13:672–676.
Stegmayr BG. Paramedian insertion of Tenckhoff catheters with three purse-string sutures reduces the risk of leakage. Perit Dial Int. 1993;13:S124–126.
Wright MJ, Bel’eed K, Johnson BF, Eadington DW, Sellars L, Farr MJ. Randomized prospective comparison of laparoscopic and open peritoneal dialysis catheter insertion. Perit Dial. 1999;19:372–375.
Yang YF, Wang HJ, Yeh CC, Lin HH, Huang CC. Early initiation of continuous ambulatory peritoneal dialysis in patients undergoing surgical implanta¬tion of Tenckhoff catheters. Perit Dial Int. 2011;31:551–557.
• Инструмент для создания подкожного туннеля не должен превышать диаметр катетера.
Crabtree JH, Fishman A, Siddiqi RA, Hadnott LL. The risk of infection and peritoneal catheter loss from implant procedure exit-site trauma. Perit Dial Int. 1999;19:366–371.
• Необходимо провести тест на проходимость катетера для перитонеального диализа для подтверждения функционирования.
• Место выхода катетера для перитонеального диализа расположено на расстоянии ≥2 см от поверхностной манжеты.
Pommer W, Brauner M, Westphale HJ, Brunkhorst R, Kramer R, Bundschu D, et al. Effect of a silver device in preventing catheter-related infections in peritoneal dialysis patients: silver ring prophylaxis at the catheter exit study. Am J Kidney Dis. 1998;32:752–760.
• Место выхода на коже катетера для перитонеального диализа направлено латерально или вниз.
Abdel-Aal AK, Dybbro P, Hathaway P, Guest S, Neuwirth M, Krishnamurthy V. Best practices consensus protocol for peritoneal dialysis catheter place¬ment by interventional radiologists. Perit Dial Int. 2014;34:481–493.
Crabtree JH, Burchette RJ. Prospective comparison of downward and lateral peritoneal dialysis catheter tunnel-tract and exit-site directions. Perit Dial Int. 2006;26:677–683.
• В месте выхода катетера для перитонеального диализа должно быть сформировано как возможно наименьшее отверстие в коже, которое позволяет пройти катетеру.
Crabtree JH, Fishman A, Siddiqi RA, Hadnott LL. The risk of infection and peritoneal catheter loss from implant procedure exit-site trauma. Perit Dial Int. 1999;19:366–371.
• Отсутствие швов на месте выхода катетера для ПД (предлагается использовать медицинский жидкий клей и стерильные клейкие полоски для закрепления катетера).
• Присоединить требуемый адаптер к катетеру и переходную трубку.
• Место выхода катетера защищено повязкой, катетер иммобилизован неокклюзионной повязкой.
Prowant BF, Twardowski ZJ. Recommendations for exit care. Perit Dial Int. 1996;16:S94–99.
John H. Crabtree, Badri M. Shrestha, Kai-Ming Chow, Ana E. Figueiredo, Johan V. Povlsen, Martin Wilkie, Ahmed Abdel-Aal, Brett Cullis, Bak-Leong Goh, Victoria R. Briggs, Edwina A. Brown, and Frank J.M.F. Dor; Сreating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 UPDATE PDI in Press. Published on April 26, 2019. Doi:10.3747/pdi.2018.00232.
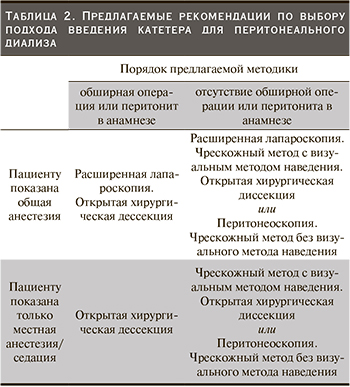
Уровни достоверности доказательств, уровни убедительности рекомендаций